

Belgium's Monkeypox "Quarantine": Historical Reaction Or Hysterical Overreaction?
It Depends On Which Meaning Of "Quarantine" You Use

Shout out to Sage Hana for calling attention to the power of words and the meanings we attach to them. It is through altered meanings that propagandists subtly shift the goalposts on just about any topic imaginable.
Yet we should be mindful also that altered meanings are not limited to just the vocabulary of COVID-19 or the Pandemic Panic Narrative. As the world grapples with a global outbreak of monkeypox, how certain words get used by the corporate media in covering the outbreak can have profound effect on the perception of the disease as well as on public health measures being introduced to mitigate the spread of the disease.
We are seeing this play out in real time with social media reactions to Belgium’s recent enacting of a compulsory 21-day "quarantine" for people infected with monkeypox.

Belgium’s compulsory measures apply only to patients with a confirmed infection. Close contacts are not required to self-isolate but are encouraged to remain vigilant, especially if in contact with vulnerable people.
“Infected persons will have to go into contact isolation until the injuries have healed (they will receive concrete instructions about this from the treating doctor),” a version of the government announcement translated from Dutch said.
The reactions to the announcement on Twitter have been eminently predictable, with numerous social media luminaries voicing their disapproval as well as fears for what Belgium’s measure signifies for the future.
Left-leaning libertarian commentator Tim Poole sees the measure as a foreshadowing of new lockdowns:

Swedish journalist Peter Imanuelson sees a repeat of 2020 beginning to unfold:
Podcaster Eric Matheny called on people to resist such measures should they happen again here in the US:
After the disastrous fiasco of the lunatic lockdowns against COVID-19 in 2020 and 2021, such reactions are hardly surprising. The lockdown strategy against COVID has failed everywhere it has been tried, and we are well advised to look askance at attempts to try it again.

However, we should also look closely at the measure being implemented in Belgium, to be sure such reactions are appropriate.
The Belgium Monkeypox Measures: What Is Really Required
The Belgium measure is simple and straightforward: if you have symptoms of possible monkeypox, see a doctor and get tested. While waiting on the test results, avoid close contact with others, and especially avoid sexual contact.
If a person develops a suspicious skin rash, the advice at this point is to contact an emergency department for sampling as soon as possible, who may refer the person to a hospital with more expertise, among others. As long as monkeypox has not been ruled out or until the infection has cleared, close contact with others should be avoided and no sexual contact is recommended.
If the test results come back positive, isolation for 21 days is required, under medical supervision.
Infected persons will have to go into contact isolation until the injuries have healed (they will receive concrete instructions about this from the treating doctor). High-risk contacts such as housemates and sexual partners are asked to self-monitor for symptoms for 21 days, taking into account the incubation period, and must not be quarantined. Contacts with pregnant women, children and immune-weakened persons are best avoided during that period.
An important point needs to be made here on language: The Belgian measure speaks to both “isolation” and “quarantine”—and, curiously enough, ultimately does not mandate “quarantine”, despite the corporate media presenting the measure as a compulsory quarantine.
To understand the distinction (and its importance), we first look to the CDC’s legal discussion on such measures for applicable definitions.
Isolation and quarantine help protect the public by preventing exposure to people who have or may have a contagious disease.
Isolation separates sick people with a quarantinable communicable disease from people who are not sick.
Quarantine separates and restricts the movement of people who were exposed to a contagious disease to see if they become sick.
The compulsory measure introduced in Belgium is in fact “isolation”. Those who are found to be infected with monkeypox are to be isolated for 21 days—essentially for the average duration of the illness so that the disease can run its course.
The Belgian measure also calls upon the partners, relatives, and other close associates of the isolated individuals to self-monitor for signs and symptoms of infection for that period, but are not formally quarantined—meaning they are not subject to compulsory isolation and restriction.
We should also understand that, whether isolation or quarantine, there is no aspect of the Belgian order which involves the sort of mass lockdowns—the compulsory restriction of movement on everyone, regardless of disease exposure—the world endured in 2020, and which in recent months turned the Chinese city of Shanghai into a Dantesque dystopian nightmare.
Whether the Belgian measures are good or bad, what they are not is indicative of lockdown: businesses are not being closed, society is not being disrupted and put on hold.
Do Quarantines Actually Work?
The practice of isolating sick individuals from the rest of the community is almost as old as civilization itself. One need only look at the proscriptions for leprosy found in Leviticus to appreciate the longevity of this public health measure. While compulsory isolation of symptomatic patients indisputably circumscribes their personal liberty, social mores have long held that to be an acceptable tradeoff against protecting the public’s health overall.
A quarantine of potentially infected individuals is both considerably more problematic and considerably more controversial. While isolating symptomatic individuals has the decided aura of “common sense”, quarantines, despite being nearly as old as isolation measures, enjoy no such credibility.
The concept of the quarantine itself traces back to the Middle Ages and the Croatian port city of Dubrovnik. After the horrors of the Black Death pandemic, trading centers like Dubrovnik needed to find a means of protecting themselves against the ravages of plague without destroying the commerce which was their lifeblood. Enter the quarantine.
Because trade with the East and the West was the driving force behind the development of Dubrovnik, suspension of trade during plague epidemics in the 14th century would have been disastrous for the city. Therefore, on July 27, 1377, the Great Council of Dubrovnik introduced in a decree a measure that would both protect against plague epidemics and free trade with eastern countries from which these epidemics usually spread. The text of this decree can be seen in Volume 78, chapter 49 of the Liber Viridis. The original document, which is kept in the Archives of Dubrovnik, states that before entering the city, newcomers had to spend 30 days in a restricted location awaiting to see whether the symptoms of plague would develop. Later on, isolation was prolonged to 40 days and was called quarantine.
The term “quarantine” is derived from the Italian word for forty, “quaranta”. We get the term from the Italian as the city of Venice, itself a maritime trading powerhouse during the Middle Ages, replicated the Dubrovnik decrees.
Perhaps in part due to the economic realities that led to the adoption of quarantine decrees, the implementation and both the real and perceived benefits of quarantine are have been found to be somewhat problematic. Sometimes quarantines are seen as successful, and other times they are seen as counterproductive.
From a historical point of view, quarantine has always been considered an effective public health measure adopted as a tool for managing infectious pathology outbreaks; in the course of time the attempt to control a large number of different transmissible diseases has involved quarantine, as has been previously illustrated for the plague, cholera, and yellow fever. In the twentieth century, other major epidemics have determined large-scale quarantine, namely tuberculosis and influenza. In the past the plague was termed the ‘Black Death’ because of its rapid insurgence, terrible epicrisis, and fatal conclusion; in the nineteenth and in the twentieth centuries, the ‘modern’ plague (the so-called ‘Great White Plague’) was considered tuberculosis (TB) (Conti et al., 2004). Use of the first powerful chemical agents against TB became widespread by the mid-twentieth century (streptomycin was put on the market in 1947). Before that date, for decades only direct and indirect quarantine measures had been implemented to contain the spread of the disease. Sanatoria and ‘preventoria’ had been established to provide preventive-therapeutic quarantine and isolation for people affected by TB. These institutions, on the one hand, represented a relatively simple instrument to set up to interrupt the pattern of transmission of this widespread pathology, and, on the other hand, they were official places where up-to-date (for the time) health care, if not effective therapy, was provided for TB patients. In the last 25 years of the nineteenth century and in the first 35 years of the following century, sanatoria spread both in North America and in Europe, with the specific function of isolating individuals affected by TB, as recommended by quarantine practice. In the absence of effective vaccines and drugs, quarantine, implemented in its broadest aspects, once again proved to be, in the case of tuberculosis in the course of the twentieth century, one of the most useful health interventions for such a widely disseminated disease.
However, from a historical and epidemiological perspective, it must also be recognized that quarantine implementation, in some of its exemplifications during the nineteenth and twentieth centuries, had unintentional negative consequences that may be illustrated by referring to some episodes in the United States (Barbera et al., 2001). One of these damaging effects was the increased risk of disease transmission in the quarantined population, as in the instance of the quarantine issued by the New York City Port Authority to prevent and contain the diffusion of cholera. In Indiana, skepticism about government recommendations for the quarantine of smallpox led to episodes of urban violence, in particular when quarantine practice was not clearly explained by the authorities to the general public. Moreover, in the case of the quarantine established in San Francisco (1900) because of a diagnosis of the plague in the Chinese neighborhood, ethic bias caused notable and exclusive detriment to the business of the Chinese community. These historical facts should be carefully borne in mind for their instructive dimension, since they constitute magisterial lessons that every contemporary health system should clearly learn.
In 2006, a mathematical modeling study of quarantine measures by Troy Day, et al, sought to address the question of when quarantines were effective, and when quarantines were likely to be ineffective. They determined that a key factor in whether or not quarantines would be effective was the reproduction rate for a particular pathogen.
In the case where R̄I > 1, quarantine is clearly necessary, and our analysis (Web appendix 2) shows that the benefit can be substantial. Now suppose that isolation alone can stop the spread of disease (i.e., R̄I < 1), so that the expected total number of infections occurring in the absence of quarantine will approach a constant value as time passes. Quarantine might nevertheless still be useful in this context by reducing the number of infections that occur before the outbreak ends.
Broadly speaking, the more contagious and transmissible a disease is, the more likely a quarantine measure will be effective at containing disease spread.
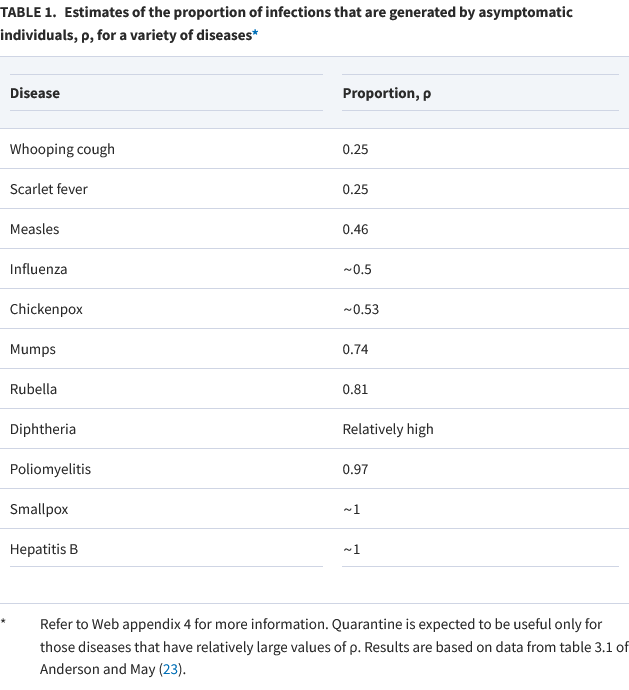
The Day study indicated there are three broad parameters which are dispositive for the efficacy of quarantine measures: a high rate of transmission, a high number of preventable infections, and the capacity and opportunity to place asymptomatic individuals into quarantine.
Our results indicate that there are three main requirements for quarantine to substantially reduce the number of infections that occur during a disease outbreak. These are the following: 1) a large disease reproduction number in the presence of isolation alone; 2) a large proportion of infections generated by an individual that can be prevented through quarantine, ρ; and 3) a large probability that an asymptomatic infected individual will get placed into quarantine before he/she develops symptoms and is isolated, q.
Thus, asymptomatic transmission of disease is an essential element of determining when quarantine is likely to be effective. Diseases such as the original SARS and influenza (and, in all probability, the entire spectrum of Influenza Like Illness, or ILI, including COVID-19), with relatively low asymptomatic transmission, are poor candidates for quarantines.
Smallpox, on the other hand, has a fairly high rate of asymptomatic transmission, and one can easily extrapolate a similar rate to monkeypox.
How Contagious Is Monkeypox?
To apprehend the likely utility of quarantine measures against monkeypox, we must be clear on how transmissible the pathogen is.
The assessment of both the WHO and the CDC is that, as human-to-human transmission requires prolonged face-to-face contact.
Human-to-human transmission can result from close contact with respiratory secretions, skin lesions of an infected person or recently contaminated objects. Transmission via droplet respiratory particles usually requires prolonged face-to-face contact, which puts health workers, household members and other close contacts of active cases at greater risk.
However, researchers at France’s Institut Pasteur have suggested that early appraisals of monkeypox contagiousness were influenced by the waning effects of smallpox immunity, courtesy of the mass vaccination campaigns which eradicated smallpox by the early 80s. As smallpox vaccines are believed to be moderately effective against monkeypox as well, the lingering effects of smallpox vaccine has, historically speaking, painted an overly optimistic picture of the transmissibility of monkeypox.
However, a complete analysis should have taken into account that, at that time, nearly all DRC population was vaccinated against smallpox and the vaccine was 85% effective against monkeypox. “We reanalyzed monkeypox historical data to assess its epidemic potential, explain Institut Pasteur researchers. Our main result is that, had the DRC population been fully susceptible to monkeypox, monkeypox would have triggered an epidemic where the average number of cases per infectious individual would have been 1.46-2.67. Furthermore, we found that low population immunity, in the range of 10-25%, may allow one infected individual to cause 1.10-2.40 new cases, and initiate an epidemic.” This is the status of many western countries, where smallpox vaccination stopped in 1980 or earlier, and immunity continued to decline, leaving the current population vulnerable to a monkeypox pandemic.
If the base reproduction number for monkeypox is ~1.46-2.67, with a high proportion of cases spread asymptomatically, the case for quarantine measures becomes fairly compelling.
Language Matters
Thus we must be clear on what is meant by “quarantine” before assessing whether a measure is prudent or not.
Mandatory isolation of patients with monkeypox has some justification, and while such measures intrinsically infringe on individual liberties, there is good reason to presume them to be an effective mitigation strategy. In any community, preventing disease spread is going to be a public priority and isolating the infected achieves that purpose. Whether that tradeoff between the public health and personal liberty is appropriate will always be a political question without a clear answer grounded in science.
A mandatory quarantine of people merely exposed to monkeypox is far more problematic. Depending on how transmissible this monkeypox strain actually is, and the proportion of asymptomatic transmission, the number of cases mandatory quarantine could prevent is less likely to be significant. However, if the base reproduction number is as high as 2.67, as has been theorized, voluntary quarantine begins to be a prudent countermeasure and mandatory quarantine becomes more defensible, particularly if monkeypox follows smallpox’ tendency towards asymptomatic transmission. Quarantines are obviously as intrinsically infringing on individual liberty as isolation, and the degree to which that infringement is an acceptable tradeoff for disease containment will always be a debate, even when quarantine measures are more likely than not to be effective.
(Side note: the low proportion of asymptomatic transmission for influenza and presumably for COVID-19 by the same logic makes quarantine largely ineffective, and the experience of the past two years bears this out).
Sadly, the corporate media (and even the alternative media) have been less than precise in their use of the term. CNBC’s reporting on Belgium’s measure simply described the effort as a quarantine, without noting the distinctions even the CDC makes between isolation and quarantine, as did the Daily Mail. Even alternative media outlet ZeroHedge failed to draw that distinction.
Yet Belgium’s public health announcement itself drew a clear distinction between the isolation measures being imposed on the demonstrably infected and quarantine measures for their close contacts, which are not compulsory. That distinction matters.
That distinction keeps the Belgian measures thus far within the realm of an historically understandable and arguably proportionate reaction to an outbreak of monkeypox, and outside the realm of an hysterical overreaction to a disease situation that does not exist.
https://tobyrogers.substack.com/p/weird-that-the-i-believe-the-sciencetm?s=r
If that’s it , full stop on the quarantine of people. It makes sense.
It’s how they should have treated Covid. But that was never the end game w Covid. Health.
The wend game as we all know is a Dictatorship of WEF.
Imagine having to listen to Klaus Schwab 24/7 on your phone, radio, TV. If you shut it off, Brown Shirt neighbors would turn you in. You know, mind F ery Hitler / Goebbels style.