“If you take Paxlovid, you might get symptoms again,” Walensky told CBS News on Tuesday. “We haven’t yet seen anybody who has returned with symptoms needing to go to the hospital. So, generally, a milder course.”
This warning comes on the heels of last week’s advisory to doctors and clinicians about the potential for rebound cases after taking Paxlovid.
A rebound of symptoms “has been reported to occur between 2 and 8 days after initial recovery,” the CDC said in an alert to healthcare providers. People who took the pill either experience symptoms or test positive for COVID-19 after having tested negative
The CDC has officially acknowledged rebound infection among COVID-19 cases and has officially blamed Paxlovid for them.
But what if they’re wrong? Could the rebound cases be the result of something else?
Rebound Cases Were Studied Long Before Paxlovid
The phenomenon of viral “rebound” is not unique to the SARS-CoV-2 virus. The phenomenon has been noted in studies of various anti-viral therapies for influenza as well as HIV.
Nor did viral rebound among COVID-19 patients emerge only with the introduction of Paxlovid. The phenomenon has appeared from the start of the pandemic.
In April of 2020, Chinese researchers Minlin Jiang, Ya Li, et al wrote a brief case study summary of 6 rebound cases (what was termed then as “recurrent PCR positivity”) that occurred between Janauary 28 and March 13 of that year, which was published in the Journal of Infection as a letter to the editor.
From the May-June, 2021, issue of Microbes and Infection there is an interesting study of 3 healthcare workers in France that displayed recurrence of COVID-19 on average over 6 months after initial recovery.
In our case series, all patients presented two episodes of SARS-CoV-2 infection separated by a symptom-free interval with a median duration between the two episodes of about 8 months.
This study stands out because of the extended period between episodes of clinical symptoms. However, study authors Souheil Zayet, Pierre-Yves Royer, et al, report that these are episodes of recurrence and not reinfection—these were not new cases of COVID-19, but a return of the initial case.
All of our patients have strong clinical and microbiological evidence that it is indeed a COVID-19 recurrence, more than the hypothesis of prolonged nucleic acid conversion in COVID-19 or traces of viral RNA.
Reports such as these are important to note because they precede introduction both of the COVID-19 inoculations and Paxlovid itself.
Simply put, rebound infection happens.
Is It Common?
How often does viral rebound happen among COVID-19 patients?
That question is somewhat more difficult to determine with any degree of precision, in part because the broad answer is “not often.” However, a study from the May, 2020, issue of the Journal of Infection followed a cohort of 55 COVID-19 patients, 5 of which developed recurrent symptoms (in this study the phenomenon was labeled “reactivation”), for a recurrence rate of 9%.
A review appearing in the European Journal of Clinical Microbiology & Infectious Diseases of several studies from 2020 showed recurrence rates ranging from approximately 1% to nearly 70%. This review contains an important caveat: the potential causes of the re-detection of the SARS-CoV-2 virus range from false RT-PCR test results to reinfection with another viral strain to actual viral reactivation. In other words, many of the studies they reviewed may represent something other than actual rebound infection/viral reactivation. One explanation they gave particular emphasis was the possibility of RT-PCR false negative test results—meaning patients truly had not recovered from infection, but were erroneously reported has having done so.
The false-negative rate of RT-PCR varies from 3 to 41%, according to the type of clinical specimen used [34, 70]. There are many reasons for false-negative RT-PCR results, including the sensitivity/specificity of the nucleic acid test kit, the sources of samples, and the sampling procedure itself [16, 71]. In a retrospective analysis involving 161 COVID-19 patients, the authors showed that false-negative test results of SARS-CoV-2 viral RNA were mainly caused by poor-quality sampling and that swabs did not contain a sufficient quantity of cellular materials [72]. Furthermore, thermal inactivation also decreases the sensitivity of RT-PCR tests for SARS-CoV-2 [73].
However, the reviews authors concluded that recurrence of the virus among recovered patients was “common”, and noted that recurrent patients were potentially contagious during the second presentation of infection.
In what appears to be the broadest survey of reinfection and recurrence among COVID-19 patients, a meta-analysis of studies from the August, 2021 issue of the Journal of Medical Virology found the rate of recurrence among recovered COVID-19 patients as 133 per 1000 patients (13.3%). Also, the study authors noted that comorbidities were prevalent among recurrent cases.
Comorbidity among recurrent cases was prevalent that the most prevalent underlying diseases among them were hypertension, diabetes, chronic respiratory diseases, liver diseases, and cardiovascular diseases.
This meta-analysis confined itself to studies from before March of 2021, which would put the actual cases primarily in 2020, thus also eliminating COVID-19 inoculation as well as Paxlovid from being influencing factors for the study.
(Update: I am guilty of transposing a decimal point here. 133 out of 1000 patients is a rebound recurrence in 13.3% of patients, not 1.33%—I moved the decimal point one place too far.
However, it must also be noted that, within the meta-analysis, many if not all of the individual studies used high cycle thresholds for establishing positive test results (Ct ≥ 37). As has been discussed by even “establishment” sources (including no less than Anthony Fauci himself), high cycle threshold values lead to higher rates of false positivity—so much so that the New York Times reported as early as August of 2020 that false positivity rates for PCR tests for COVID-19 are as high as 90%, meaning only 1 out of every 10 positive test results represents an actual case of COVID-19.
Thus, while I made an immediate math error, there is also an arguable logical error in the meta-analysis that cancels out the math error, as we should be prepared to discount 90% of the positive RT-PCR tests used to establish viral rebound, making the 133 out of 1000 patients a likely overstatement of actual viral rebound, and leading us back to a percentage of ~1-2%, making 1.33% still the “best estimate” for actual viral rebound. That 90% overstatement is a figure that can be supported from multiple independent sources, and even the CDC has conceded the hyper-sensitivity of RT-PCR tests with high cycle thresholds.)
The “best estimate” we seem to have for viral rebound among COVID-19 patients, therefore, before inoculation and Paxlovid treatment come into the picture, was around 1.33% of cases, with most cases involving at least one comorbid condition.
Rebound Happens When The Body Fails To Clear The Virus
A rather obvious point must be emphasized here: viral rebound occurs when the body fails to clear the virus. Even though symptoms may recede, active virus is still present within the body and thus can potentially stage a comeback.
Why does the body fail to clear the virus? The particulars of that question are not something that mere data analysis can answer, although the prevalence of comorbidities is an important indicator of what is happening broadly speaking in the body: the immune system is not sufficiently robust to clear the body of active virus.
As I noted last December, studies showing better inoculation results among patients with no comorbidities also showed, as a result, that comorbidities are a rough metric for immune system dysfunction:
Another implication of this correlation is that comorbidities weaken the immune system and are themselves an indicator of a level of immune system dysfunction. The greater the dysfunction the less effective the vaccines.
Thus, even patients technically not classified as immunocompromised but presenting with one or more significant comorbidities are to some degree immunodeficient.
That a weaker immune system will have a greater challenge in achieving full viral clearance is intuitively obvious.
Rebound Cases Undercut The Argument For Paxlovid Efficacy
The reality of viral rebound also provides yet more evidence that Paxlovid is not effective in getting rid of the SARS-CoV-2 virus.
In studies, Pfizer reported that 1% to 2% of people taking the medication experienced rebound. The company says the rates of rebound in the treated group in its study and among those receiving placebo were similar, indicating that “elevated nasal viral RNA is uncommon and not uniquely associated with treatment.”
A 1-2% rebound rate among Paxlovid trial patients lines up with the existing research supporting a broad viral rebound recurrence rate of 1.33%. Pfizer even admits that the rates of rebound between the treatment arm and the placebo arm of the clinical trial were “similar”.
However, this means that Paxlovid itself is not accomplishing anything more than suppressing COVID-19 symptoms.
Clinical trial subjects are meant to represent a broad cross-section of the overall patient population, and both the treatment and placebo arms of any study should involve patient cohorts that are as nearly identical as possible. Therefore, if rebound rates are similar between the Paxlovid treatment arm and the placebo arm, and both are in line with previously established estimates for viral rebound, the drug by definition is having zero impact on viral clearance. If there were positive impact on viral clearance, the Paxlovid rebound rates should be lower than naturally occurring rebound rates; instead, the rates are approximately the same.
Studies of rebound cases also through a bit of shade on Pfizer’s claim of efficacy at preventing hospitalization. A case study of 10 rebound cases by Michael Charness and Kalpana Gupta, both of the VA Boston Healthcare System, et al, noted that, while none of the 10 cases required hospitalization during the rebound episode, they also were not hospitalized initially.
Relapse symptoms were milder than presenting symptoms in 7 of 10 cases, and fever was notreported. No patient required urgent care, emergency room, or hospital care during initial or relapsesymptoms, and all patients recovered without additional antiviral treatment. Antigen tests during relapsebecame strongly positive on Days 9-13 (median Day 10) and remained so for at least 2 to 7 days (median6 days; not measured daily) until as late as Day 18, well past the recommended period for isolation.
As the rebound episode was not treated with additional Paxlovid, we have a rough comparison per patient of the disease with and without Paxlovid, and while the 10 cases were milder during the rebound episode, the lack of hospitalization of any of them raises the question of whether hospitalization would have occurred without Paxlovid during the initial period of infection.
We cannot answer that question on rebound cases alone, as an exact comparison of initial and rebound episodes is invalid for multiple reasons—not the least of which is the time frame for the immune system to be working on the virus—but if the sole benefit of Paxlovid is staying out of hospital, that benefit disappears if the patient was never going to be in hospital anyway. The untreated rebound episodes in the Charness study present at least the possibility that this was the case for those 10 patients.
The Vaccinated Fare Worse
Yet Paxlovid rebound presents another and far more disturbing problem: while there are no formal clinical studies to substantiate this, multiple doctors—including those who agree with the administration of Paxlovid—are asserting that the rate of rebound is far greater than the naturally occurring 1-2%.
But a growing number of people are reporting infection rebounds after taking Paxlovid—so many that “there’s no way it’s occurring at 1% or 2%,” says Ho, who has also shared his data and discussed it with scientists at Pfizer. “It’s happening quite a bit.”
The real number is—well, we have pretty much no idea what the real number is. The federal government is not tracking Paxlovid rebound in any public-facing database, and the CDC released an advisory on Tuesday saying the agency doesn’t know whether a recurrence of symptoms can be connected to the drug. The agency also clarified that “Paxlovid continues to be recommended for early stage treatment of mild to moderate COVID-19 among persons at high risk for progression to severe disease” and that anyone who rebounds should isolate for another five days. No researchers have yet published studies measuring the prevalence of rebound, but a good number of clinicians and Paxlovid patients are convinced that it’s higher than 2 percent. “To trust that number would’ve been to not believe my eyes,” Bob Wachter, the chair of medicine at UC San Francisco, told me.
In an attempt to find some clarity, Wachter decided to poll his Twitter connections on whether they’d taken Paxlovid and rebounded. (I’m legally obligated to tell you that Twitter polls are neither scientific nor particularly reliable—which Wachter knows perfectly well.) Of the respondents who said they had taken Paxlovid, 45 percent rebounded; Wachter said he guesses the real proportion is closer to 10 or 20 percent. A few hours after we spoke, Wachter tweeted that his wife, who had recently finished a course of the antiviral and recovered from COVID, just tested positive again.
One common factor among the studied rebound cases: the patients were inoculated and in most cases boosted as well.
The 10 patients in the Charness study were “fully vaccinated” (i.e., inoculated—let us not lose sight of the reality that the COVID shots are not vaccines).
The four patients (1 rebound) in the Carlin study at UC San Diego were “boosted”.
Here is the conundrum: If Paxlovid plays little or no role in viral clearance—as Pfizer’s own attestation of its clinical results suggest, and as comparison to earlier studies of viral rebound indicate—and if the “natural rate” of viral rebound among COVID patients prior to the mass administration of the COVID inoculations is ~1-2%, how is it that Paxlovid rebound cases—the majority of which appear to be at least inoculated and many are inoculated and boosted—are as high as 10-20%?
If we proceed from the presumption that Paxlovid plays little or no role in viral clearance, then the higher incidence of “Paxlovid rebound” cases leads to a very disturbing conclusion:
Patients who are inoculated against COVID have greater difficulty clearing the virus than patients who are not.
At a minimum, we have the possibility that Paxlovid somehow retards viral clearance, although the broad equivalence of viral rebound among non-inoculated Paxlovid patients from the clinical trials with the natural rate of viral rebound (both historically and from Pfizer’s own placebo arm) argues against that possibility (if that were happening, rebound cases would be higher among the Paxlovid patients). If the Pfizer data is to be trusted (which is a Mount Everest-sized “if” on a good day), Paxlovid is not likely to be retarding viral clearance.
If Paxlovid is not retarding viral clearance, then the inoculations must be.
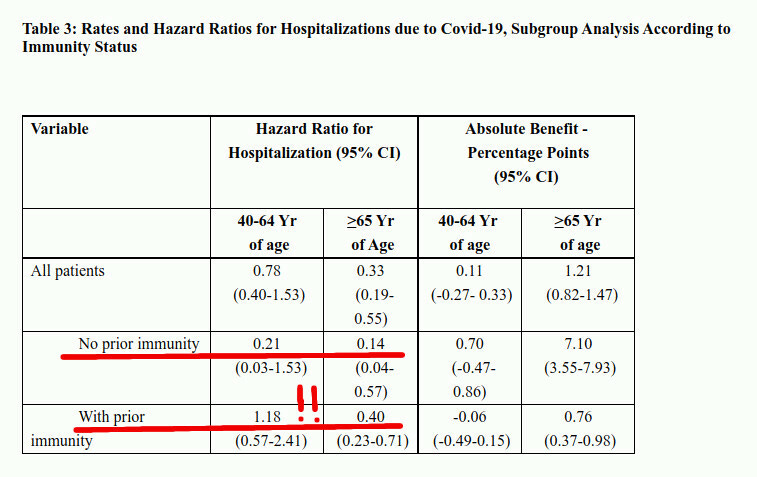
The rebound infection data, sparse though it is, aligns well with other more formal studies which, as Igor Chudov documents (his latest article came out as I was writing this!), indicating that patients with “prior immunity” (i.e, inoculated) are at greater risk of hospitalization than patients who were not.
What is it showing? Look at the first underlined line, “no prior immunity”. You will see that for people with “no prior immunity”, Paxlovid works fairly well.
For example, for younger 40-64yo “no prior immunity” patients, Paxlovid-treated persons have only 0.21 times the risk of untreated patients. For the older over-65 years old group, the risk for Paxlovid-treated patients is only 14% of the no-Paxlovid group. For the unvaccinated (no-immunity, see discussion above) Paxlovid works a little worse than in the Pfizer-sponsored EPIC-HR trial, but still decently.
The shocker lies in the vaccinated group! Paxlovid does NOT work at all — and shows INFERIOR RESULTS — in the younger 40-64 unvaccinated subgroup. In fact, the small statistical sample shows that the risk of severe outcomes in the Paxlovid group is HIGHER than in the no-Paxlovid group (1.18). The sample is relatively small, but you can see that for younger vaccinated persons, Paxlovid is at best useless, and at worst, harmful.
When two independent paths of investigation reach a similar conclusion, the technical term for that is “confirmation”.
The Israeli study Igor dissects aligns extremely well—disturbingly well—with rebound infection data in confirming that vaccinated patients fare worse than unvaccinated patients.
Whatever benefit Paxlovid has in ameliorating symptoms for the duration of the drug’s administration, it cannot mask the reality that inoculated individuals are exhibiting significant increases of immune system dysfunction.
I will restate for emphasis the argument I made last December regarding inoculation efficacy:
Another fascinating statement in the study is the acknowledgement that healthier individuals have better outcomes from vaccination.
Although risk for a breakthrough infection increased with greater number of comorbidities, this risk was associated with and notably attenuated by immune dysfunction status.
While such a correlation is on its face unsurprising, we should remember that the healthy patient population is already at the lowest risk from COVID-19. Vaccines which are effective only for healthy individuals are of questionable practical utility, given that less healthy individuals are the ones at greatest risk and in need of the most protection.
Another implication of this correlation is that comorbidities weaken the immune system and are themselves an indicator of a level of immune system dysfunction. The greater the dysfunction the less effective the vaccines.
In the ultimate medical perversity, Paxlovid reveals inoculation status to be itself an identifiable co-morbidity for COVID-19 cases.
The CDC Mis-States The Situation
Rochelle Walensky’s May 31 statement to CBS News focuses attention on Paxlovid. However, she omitted an arguably more important reality: While there is a potential for viral rebound after taking Paxlovid, there is a greater potential if one is inoculated.
She is not likely to make that second statement, of course, because to do so would be to acknowledge that the inoculations have demonstrably damaged people’s immune systems—something that we arguably can see from broader epidemiological data showing that people today are sicker overall than they were before the pandemic, the lockdowns, and especially the inoculations.
The statement Ms. Walensky should be making should read something like this:
"Paxlovid is an antiviral that suppresses symptoms of COVID-19, but does not help your body get rid of the virus. If you are among the fully inoculated and boosted, Paxlovid merely masks the reality that your body is less able to get rid of the virus than before you received the inoculation.”
To be sure, Ms. Walensky has not made a statement even remotely like this, and is not likely to do so in the future. No one who has had a hand in spreading the damnable lie about inoculation efficacy is going to admit the shots’ provable (and proven) toxicities.
Yet as time passes, we see more and more evidence the inoculations are indeed quite toxic. The greater prevalence of viral rebound among inoculated patients taking Paxlovid than among non-inoculated patients is merely one more nail in the inoculation coffin.
The COVID-19 inoculations do harm to people, and Paxlovid proves it.
The problem is that people are educated just enough to believe what they have been taught, and not educated enough to question anything from what they have been taught.
Igor and Brian Mowrey have been posting about Paxlovid for a while. During the Paxlovid trial, only some of the participants were tracked via PCR, and I believe it was around 12% showed a viral spike in the second week. It appears Pfizer came up with the 1-2% number by dividing the number of rebound cases (which were only discovered through a small sampling of the participants) by the total number of participants.





The problem is not people being uneducated.
The problem is that people are educated just enough to believe what they have been taught, and not educated enough to question anything from what they have been taught.
Richard Feynman
Igor and Brian Mowrey have been posting about Paxlovid for a while. During the Paxlovid trial, only some of the participants were tracked via PCR, and I believe it was around 12% showed a viral spike in the second week. It appears Pfizer came up with the 1-2% number by dividing the number of rebound cases (which were only discovered through a small sampling of the participants) by the total number of participants.