

Ignorance Is Not Bliss: The Legacy Media Is Both Incompetent And Dishonest About CCPVirus Treatments

We must not be surprised when politicians engage in hyperbole. For better or worse, it is a staple of political rhetoric--everything they do is "the best" and everything their opponents do is "the worst". This has been true of politics dating back to the Roman Republic.

We can therefore be reasonably skeptical when President Trump's Press Secretary, Kayleigh McEnany, describes FDA authorization of Convalescent Blood Plasma as a "breakthrough". We should expect such hyperbole for every bit of good news coming from any President's administration.

We should be far less forgiving, however, of the legacy media treating the hyperbole with a strange naivete, especially when choosing to downplay both the announcement and the significance of the treatment option. Convelscent Blood Plasma may be many things, but what no treatment that has been around for nearly 160 years can be called is a "breakthrough"--and it beggars belief that the legacy media remains studiously unaware of this fact.
Convalescent Blood Plasma: The Non-Breakthrough "Breakthrough"
The "breakthrough" announcement first appeared on Twitter late in the evening on Saturday, August 22, when Press Secretary McEnany promised a "breakthrough" announcement in the Sunday press briefing.
News conference with President @realDonaldTrump at 6 pm tomorrow concerning a major therapeutic breakthrough on the China Virus. Secretary Azar and Dr. Hahn will be in attendance.
— Kayleigh McEnany (@PressSec) August 23, 2020
That "breakthrough" was later reported to be new FDA authorizations regarding Convalescent Blood Plasma (CBP) as a treatment option for CCPVirus cases.
President Trump is expected to announce Sunday evening that the Food and Drug Administration will authorize the use of blood plasma from patients who have recovered from Covid-19 as a treatment for the disease, according to an individual familiar with the plans.
The decision, which Trump’s press secretary heralded ahead of time as a “major therapeutic breakthrough,” likely falls far short of that description — and could generate intense controversy inside the administration and the broader scientific community.
What was left unsaid in the report is not only that CBP has been used for CCPVirus treatments for quite some time as it is, but that the treatment regimen itself is over a century old.
From the 1880s to the antibiotic era, CBP were used to prevent and treat many bacterial and viral infections in humans and in animal models. In 1890, the first rational approach exploited by the physiologists von Behring and Kitasato to treat diphtheria was blood serum; initially, it was produced from immunised animals but soon whole blood or serum from recovered donors with a specific humoral immunity were identified as a possible source of specific antibodies of human origin. There are several examples of the use of CBP for the prophylaxis or treatment of bacterial infectious diseases such as scarlet fever in the 1920–40s and pertussis until the 1970s.
Far from being a "breakthrough", CBP is one of the oldest medical treatments since the advent of germ theory in the mid-19th century.
This historical backdrop matters. The history of CBP is itself a demonstration that while new treatments may prove more effective than older ones, treatments that have worked in the past do not stop working just because newer treatments are available. The context that is unforgivably absent from the legacy media reporting is that the medical arsenal expands over time, and is almost never entirely empty.
The history of CBP and its survival as a treatment option through the 20th century also attests to its fundamental efficacy. Treatments need not be "magic bullets" to be effective, and CBP, while not a magic bullet, has proven itself in a variety of treatment scenarios.
The FDA Has Already Authorized CBP
Moreover, the legacy media largely ignores even the recent history of CBP, which was authorized by the FDA for experimental use all the way back on March 26.
Because COVID-19 convalescent plasma has not yet been approved for use by FDA, it is regulated as an investigational product. A health care provider must participate in one of the pathways described below. FDA does not collect COVID-19 convalescent plasma or provide COVID-19 convalescent plasma. Health care providers or acute care facilities would instead obtain COVID-19 convalescent plasma from an FDA-registered blood establishment.
To be sure, experimental, or "investigational" use is not the same as authorization for broad general use, but surely it is relevant to know that CBP has been considered as a treatment option for CCPVirus for quite some time.
At the height of the New York City outbreak, in April, the use of CBP was touted as a potential "game changer".
Dr. Jeffrey Jhang, medical director of clinical laboratories and transfusion services for the Mount Sinai Health System, said: "We have so many patients who are sick. We are crossing our fingers that this will be a game changer and really accelerate the recovery of these patients."
It should be noted that this particular article did give a brief summary of the diseases treated with CBP over time, but it is by far the exception.
Do Not Forget Hydroxychloroquine
No discussion of legacy media ineptitude on CCPVirus would be complete without mentioning hydroxychloroquine. Hydroxychloroquine, and its close cousing chloroquine phosphate, were among the earliest drugs approved by China for treating CCPVirus, receiving approval in mid-February.
This early adoption of chloroquine should surprise no one. Quinine, the naturally occurring analog to chloroquine and hydroxychloroquine, was first examined as a treatment for respiratory illness as far back as 1889, and chloroquine was specifically studied for use against SARS in 2004. There are, at present, 79 studies on the efficacy of hydroxychloroquine against CCPVirus, 46 of which have been peer-reviewed. The data on hydroxychloroquine is positive, to say the very least:
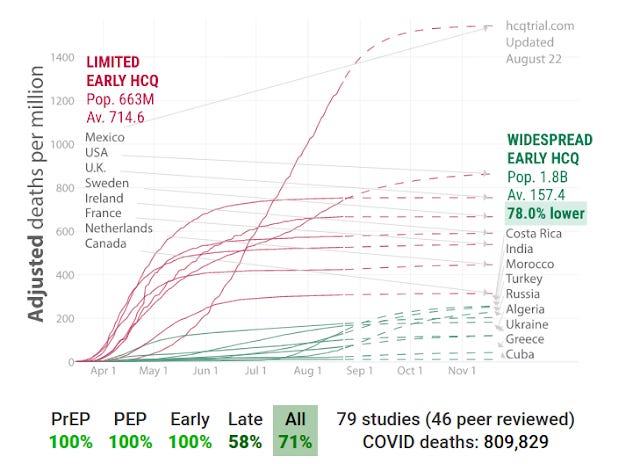
As an early treatment for CCPVirus, as well as for pre-exposure and post-exposure prophylaxis, hydroxychloroquine shows considerable promise--and could arguably claim "magic bullet" status.
However, according to the legacy media, there is "no evidence" that hydroxychloroquine works.
As some global leaders tout the effectiveness of hydroxychloroquine against COVID-19, scientists from those countries caution that there’s not much evidence it works, putting the drug at the center of political debate.
It is empirical fact that 79 studies, on balance, say otherwise. It is equally empirical fact that quinine, upon which hydroxychloroquine is based, has a lengthy and documented history as a treatment for respiratory illness. Yet the media presents hydroxychloroquine as a drug with no connection to quinine or any history as a therapy for respiratory illness.
Hydroxychloroquine is an immunosuppressive drug that was developed decades ago to prevent and treat malaria. It’s also used to treat autoimmune diseases like systemic lupus erythematous and rheumatoid arthritis.
Such depictions ignore the empirical fact of in vitro studies of chloroquine which showed promise against SARS as well as MERS.
Almost daily we see articles throughout the legacy media which declaim the efficacy of hydroxychloroquine.
In the Daily Mail.
On NBCNews.com.
In the Detroit Free Press.
In the New York Times.
Nowhere in the legacy media treatments of hydroxychloroquine is there any mention of the extant body of research on hydroxychloroquine and chloroquine as coronavirus therapies. It is one thing to challenge the conclusions of various research studies, but it is quite another to pretend those studies do not exist.
The legacy media is demonstrably dishonest in its discussion of hydroxychloroquine simply by virtue of its (willful?) ignorance of the totality of research on the topic. If they are demonstrably dishonest in that regard, we are compelled to inquire into what other aspects of their reporting might be factually false or even dishonest. We are precluded from granting the legacy media reporting any semblance of trust because of their obvious intellectual lassitude.
The Promised Magic Bullet: Vaccines
Both the legacy media and the self-anointed disease "experts" around the world are quick to promise a "magic bullet" for CCPVirus, and that is a vaccine.
So certain are they of the efficacy of a vaccine the experts are quite emphatic that everyone must be compelled to take it, that it should be illegal to refuse it.
If and when a coronavirus vaccine is rolled out, there will be people who refuse to take it for various reasons, but a Stanford Law School professor says such refusal will have consequences.
This argument is made even with the acknowledgment that the first vaccines will be only 50% effective.
An approved coronavirus vaccine could end up being effective only 50-60% of the time, meaning public health measures will still be needed to keep the pandemic under control, Dr. Anthony Fauci, the top U.S. infectious diseases expert, said on Friday.
"We don’t know yet what the efficacy might be. We don’t know if it will be 50% or 60%. I’d like it to be 75% or more," Fauci said in a webinar hosted by Brown University. "But the chances of it being 98% effective is not great, which means you must never abandon the public health approach."
The presumed "top expert" on infectious diseases is suggesting that the initial CCPVirus vaccines will be only 50% effective, and yet that is enough to coerce everyone to be vaccinated.
Why is this a problem? It is a problem because no matter how solid the scientific theory behind a particular vaccine or vaccine technology might be, each vaccine is itself a product, and products may be badly manufactured and capable of doing far more harm than good.
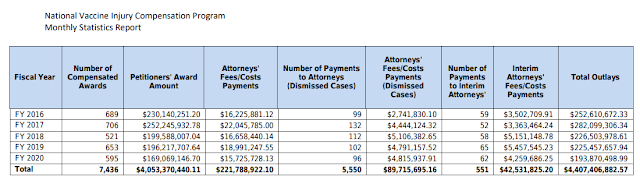
This is not idle speculation. The United States maintains a fund--the National Vaccine Injury Compensation Program--which compensates people for harm inflicted by an errant vaccine. Since the program's inception, it has paid out over $4.4 billion, and in the past four years it has paid out between $200 and $250 million every year.
Unsurprisingly (yet sadly) there is no mention of these documented facts in the legacy media coverage of efforts to develop a CCPVirus vaccine. This despite ample coverage of vaccine development by the legacy media:
There is no mention of VICP on Yahoo!
There is no mention of VICP in USAToday.
There is no mention of VICP on CBS.
There is no mention of VICP in the Madison State Journal.
There is no mention of VICP in Newsweek.
We have documented proof of the very real potential for vaccines to cause injury, yet this is not being discussed anywhere in the legacy media.
Nor do we see much if any discussion of the recent research project conducted at Yale to determine what persuasion techniques should be used on various demographics to ensure maximum compliance with a vaccination program.
Nor do we see much exploration of the liability waivers being granted by every nation to Big Pharma for their CCPVirus products.
A senior executive from AstraZeneca, Britain's second-largest drugmaker, told Reuters that his company was just granted protection from all legal action if the company's vaccine led to damaging side effects.
Or that such immunities are part of the legislative backdrop for vaccine development in the United States.
As for the US, well, when it comes to the legal framework around vaccines, the US Food and Drug Administration (FDA) already has a law called the Public Readiness and Emergency Preparedness (PREP) Act, which provides immunity to vaccine companies if something goes wrong.
Pharmaceutical companies are in an all out race to develop vaccines for CCPVirus, and yet the legacy media is not considering or presenting the risks associated with these coming products. Even though the FDA must approve all vaccines, we must remember that, even with FDA approval, the United States still pays out over $200 million to settle vaccine-related injury claims every year.
We are not told this by the legacy media.
Context Matters
When discussing any topic, or presenting any news story, framing matters. Historical background and the existence of other data which presumably challenges a particular narrative are but a few of the elements an honest presentation any topic demands. At a minimum factually false claims and inferences must be avoided.
These are not standards to which the legacy media adheres, certainly not as regards CCPVirus treatments.
Yet without context, without historical background and the awareness of all the extant data, we cannot hope to have rational discourse about anything. We cannot rationally conceptualize the severity of the CCPVirus, nor can we adequately assess for ourselves the risks and benefits of various treatment modalities.
Without context, what otherwise would be objective reporting is reduced to mere propaganda and narrative, neither of which serves the public's interests at all.