

OSHA Emergency Temporary Standard On COVID Vaccinations Contradicts Reality
The OSHA Mandate Gets The Facts Very, Very Wrong


OSHA has now released its Emergency Temporary Standard requiring virtually all employers to coerce their employees to receive one of the available COVID-19 vaccinations (Pfizer, Moderna, and Johnson & Johnson). As expected, its rationale lacks one essential element: factual support.
Readers will recall just last month I laid out the basic case against this OSHA rule, pointing out how the facts surrounding COVID-19 in the United States simply did not support President Biden’s assertions from his September 9 speech announcing his intent to seek this rule. Those facts remain. They have not changed, other than for additional data to amplify the fundamental irrationality of the new OSHA mandate.
Most recently, I highlighted how, in highly vaccinated country after highly vaccinated country, the vaccines have failed utterly to prevent new waves of coronavirus infection.
It is against this backdrop that we must read and review the OSHA Emergency Temporary Standard.
Assertion: Workers Are Contracting COVID
The essential rationale for the ETS is that COVID-19 is a threat to America’s workers in the American workplace.
At the present time, workers are becoming seriously ill and dying as a result of occupational exposures to COVID-19, when a simple measure, vaccination, can largely prevent those deaths and illnesses.
Against this rationale, consider the facts:
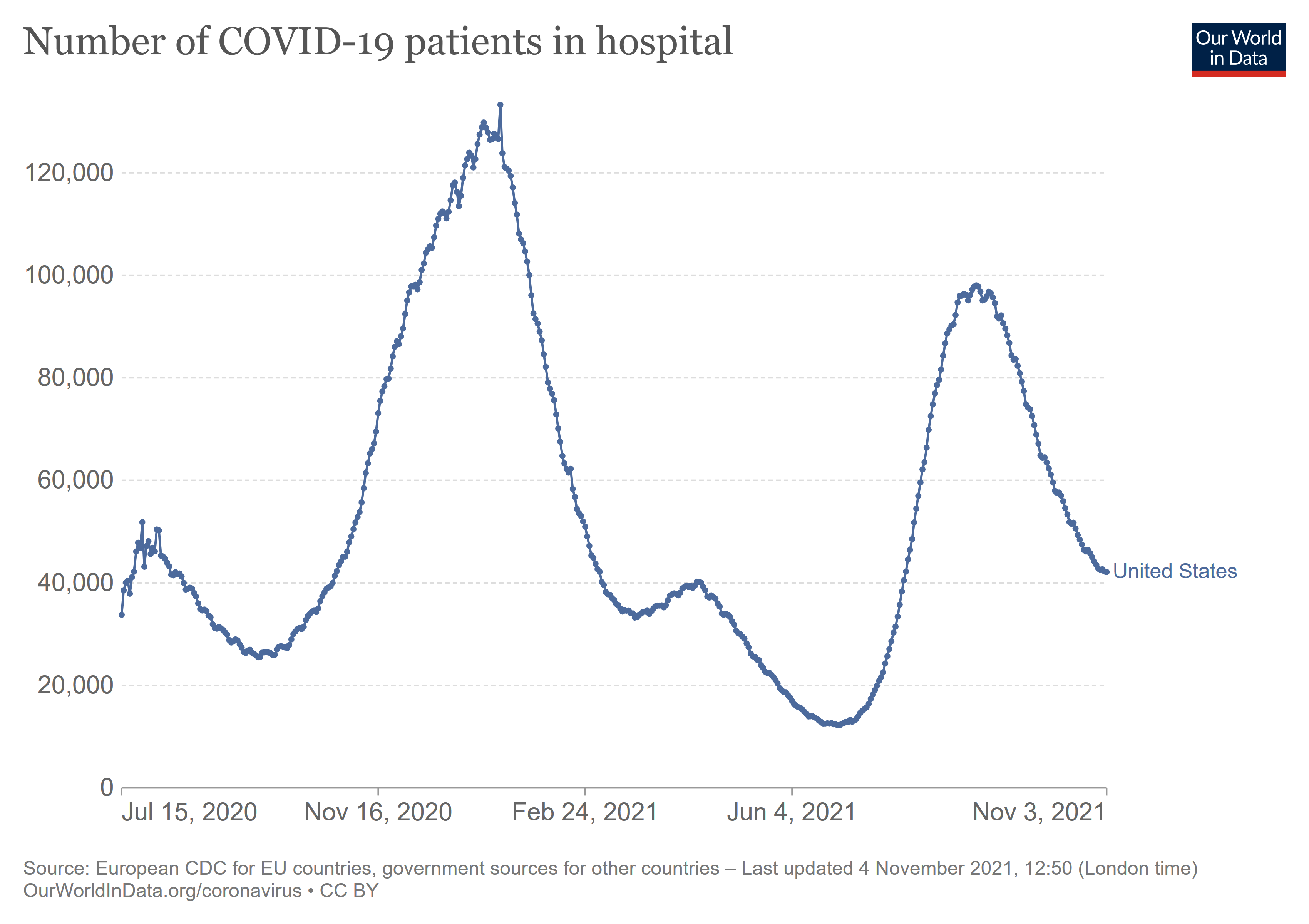
As of November 2, 2021, there are 42,221 patients in the US reported as hospitalized for COVID-19 infections. This is less than half of the most recent peak for such hospitalizations (September 2) of 97,811, and barely a third of the January 15 peak of 123,790. Moreover, the trend has been uniformly down since September 2.
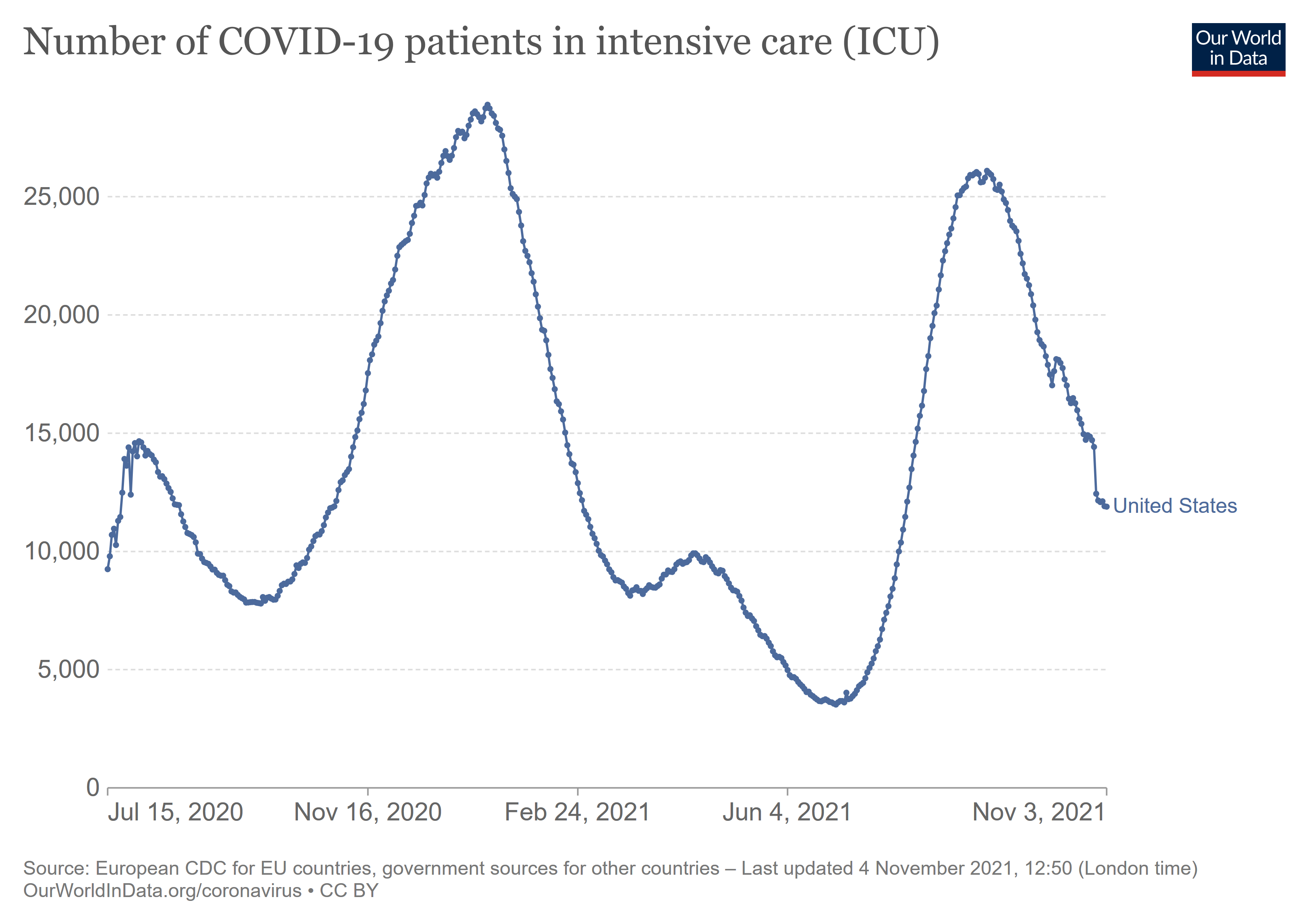
Slightly more than one fourth (11,914 as of November 2) of those patients are in ICU, and that trend is also on a steady decline.
Americans, not just workers, are quite clearly not getting “seriously ill” with COVID-19 at this time.
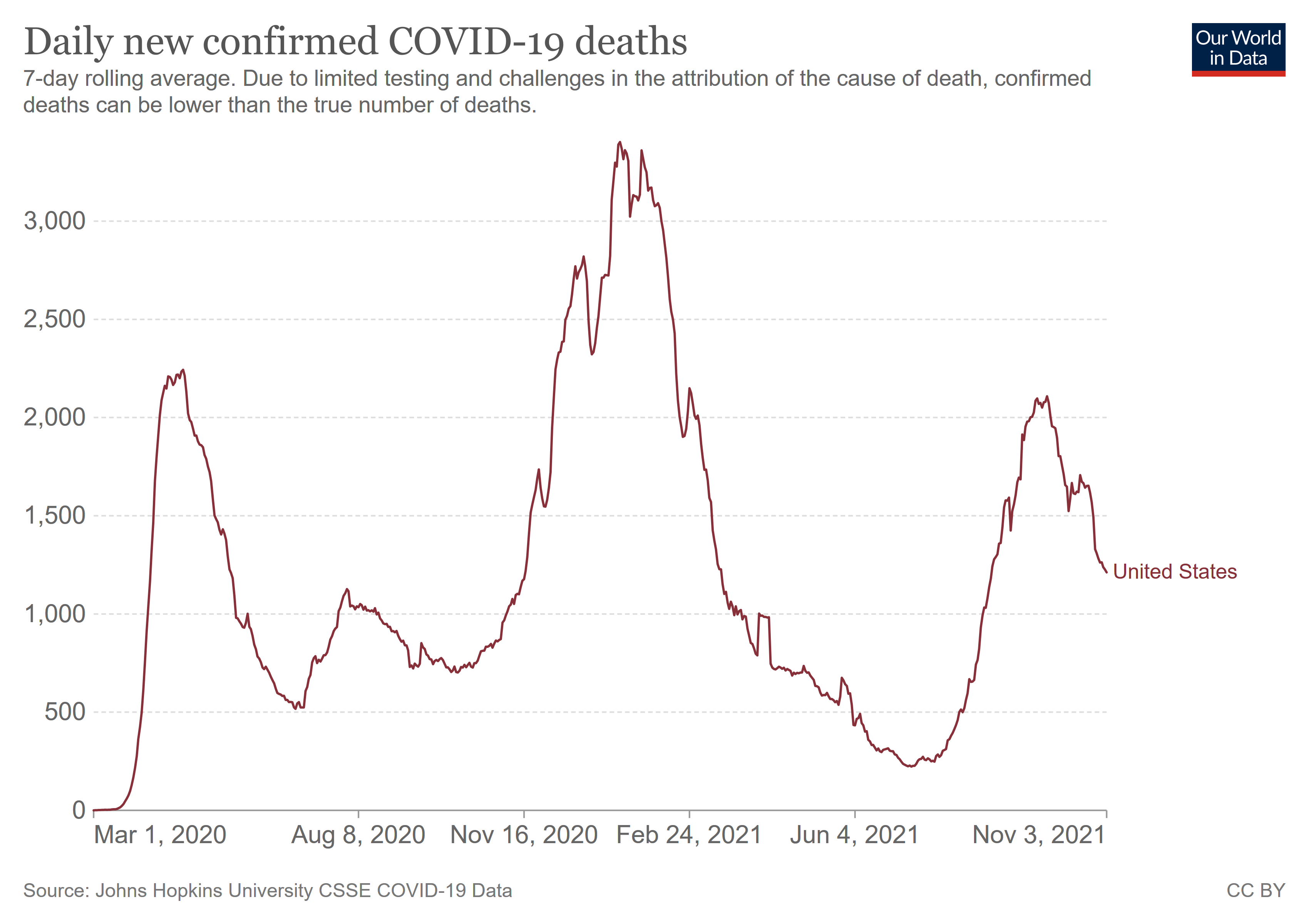
Nor are they dying. The seven-day average for COVID-19 deaths in the United States is 1,226.43 as of November 2. The US has a population of over 330 million.
According to government data, in 2020 there were 2.7 million non-fatal workplace injuries and illnesses—injuries and illnesses that are already covered by OSHA regulations.
At a minimum, OSHA is wasting precious resources chasing COVID-19 cases when there are 2.7 million existing opportunities to improve existing safety mandates and systems.
Assertion: COVID-19 Infection Occurs Primarily In The Workplace
The ETS rationale further presumes that COVID-19 infection is mainly a workplace phenomenon.
OSHA has determined that many employees in the U.S. who are not fully vaccinated against COVID-19 face grave danger from exposure to SARS-CoV-2 in the workplace.
However, researchers established literally at the outset of the pandemic in the US that the riskiest place for COVID-`9 infection was the home.
As seven states now require masks and face coverings for visiting essential businesses or using public transportation, it seems like those spaces are where we are most at risk for COVID-19 infection. But, in truth, the riskiest place could be our homes — at least, if you live with someone who tests positive for the virus. That’s why Jessica Lin, an infectious disease researcher at the University of North Carolina at Chapel Hill, is leading a study to address the infection rates of household members living with someone who has tested positive for COVID-19.
Subsequent research has continued to affirm this characteristic of COVID-19 infection.
Households showed the highest transmission rates, with a pooled SAR of 21.1% (95% confidence interval [CI]:17.4–24.8). SARs were significantly higher where the duration of household exposure exceeded 5 days compared with exposure of ≤5 days. SARs related to contacts at social events with family and friends were higher than those for low-risk casual contacts (5.9% vs 1.2%). Estimates of SARs and Robs for asymptomatic index cases were approximately one-seventh, and for presymptomatic two-thirds of those for symptomatic index cases. We found some evidence for reduced transmission potential both from and to individuals younger than 20 years of age in the household context, which is more limited when examining all settings.
The most probable avenues of infection have been and continue to be the close contacts of friends and family, and not the more casual contacts of the workplace. To the extent that workers anywhere are at risk of COVID-19 infection, that risk lies largely outside the workplace.
OSHA has ZERO authority to regulate anything outside the workplace. Based on the evidence, that include COVID-19 infections.
Assertion: Vaccination Will Prevent COVID
The ETS rationale also presumes that vaccination will prevent COVID-19 illness.
At the present time, workers are becoming seriously ill and dying as a result of occupational exposures to COVID-19, when a simple measure, vaccination, can largely prevent those deaths and illnesses.
As the experiences of Ireland, Israel, Germany, New Zealand, and Singapore demonstrate, the vaccines do not prevent COVID.
A brief inspection of Ireland and Israel’s hospitilization data shows the vaccines also do not prevent hospitalizations, with both countries experiencing a rise in hospitalizations since July.
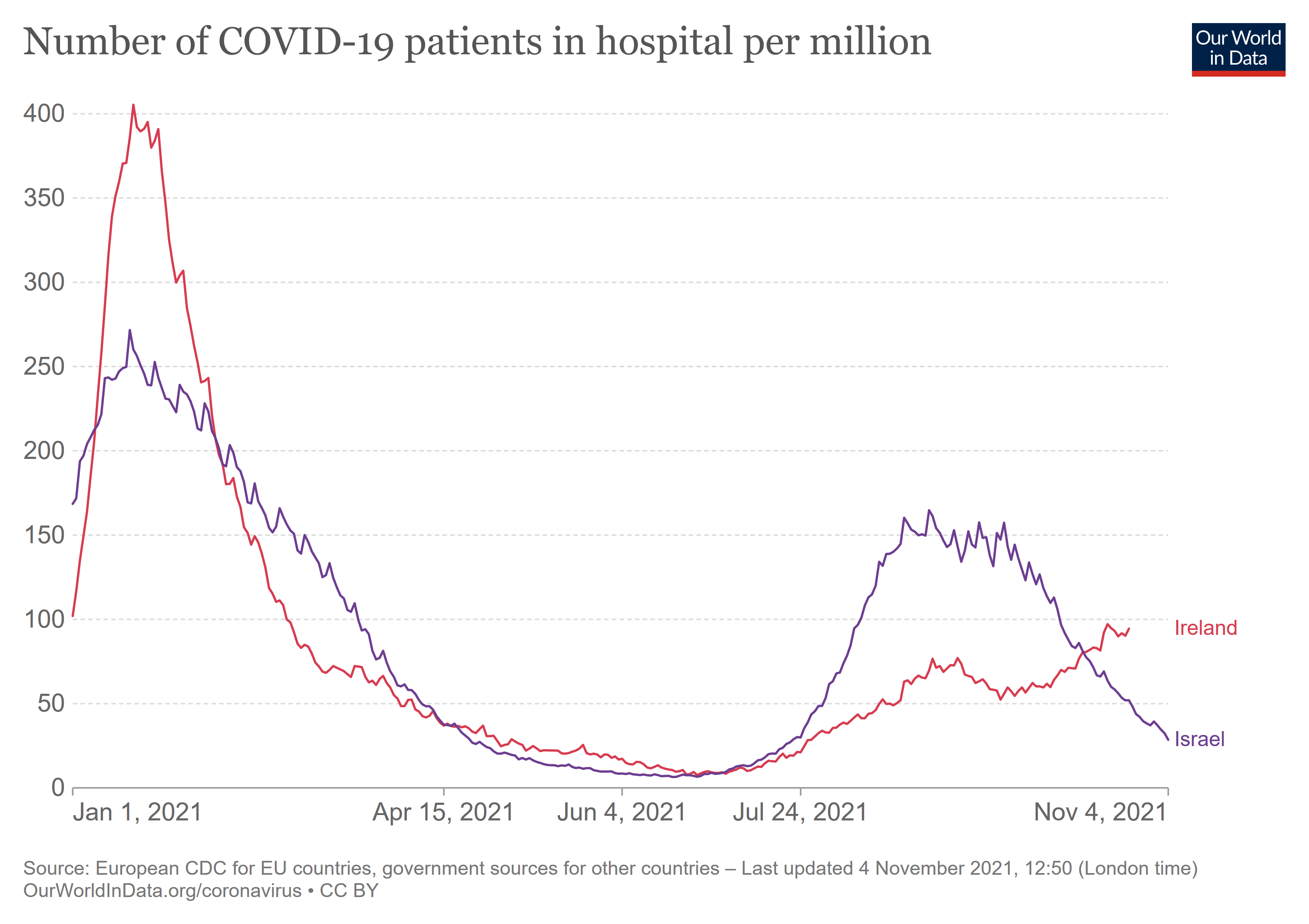
For the OSHA ETS to make sense, these recent waves of hospitalizations should not have happened. But they did.
Assertion: There Is No Natural Immunity To COVID
Among the most surprising assertions made by OSHA is the outright denial of natural immunity arising from prior COVID-19 infection.
OSHA determined that workers who have been infected with COVID-19 but have not been fully vaccinated still face a grave danger from workplace exposure to SARS-CoV-2.
This is, to put it kindly, nonsense. Even the National Institutes of Health has established that natural immunity to COVID-19 arises from COVID-19 infections.
We analyzed multiple compartments of circulating immune memory to SARS-CoV-2 in 254 samples from 188 COVID-19 cases, including 43 samples at ≥ 6 months post-infection. IgG to the Spike protein was relatively stable over 6+ months. Spike-specific memory B cells were more abundant at 6 months than at 1 month post symptom onset. SARS-CoV-2-specific CD4+ T cells and CD8+ T cells declined with a half-life of 3-5 months
The WHO’s May 10 Scientific Brief on natural immunity carried the same positive message.
The strength and duration of the immune responses to SARS-CoV-2 are not completely understood and currently available data suggests that it varies by age and the severity of symptoms. Available scientific data suggests that in most people immune responses remain robust and protective against reinfection for at least 6-8 months after infection (the longest follow up with strong scientific evidence is currently approximately 8 months).
As a September article in TheBMJ points out, infectious disease researcher Monica Gandhi at the University of California/San Francisco had been assembling a list of research studies documenting natural immunity, stopping when the list simply became too long to manage.
Gandhi included a list of some 20 references on natural immunity to covid in a long Twitter thread supporting the durability of both vaccine and infection induced immunity. “I stopped adding papers to it in December because it was getting so long,” she tells The BMJ.
But the studies kept coming. A National Institutes of Health (NIH) funded study from La Jolla Institute for Immunology found “durable immune responses” in 95% of the 200 participants up to eight months after infection. One of the largest studies to date, published in Science in February 2021, found that although antibodies declined over 8 months, memory B cells increased over time, and the half life of memory CD8+ and CD4+ T cells suggests a steady presence.
The best available evidence indicates that people who have been previously infected with COVID-19 are not in grave danger. OSHA’s assertion here is simply false.
If OSHA’s Assertions Are Wrong, So Is The ETS
Setting aside for this discussion the legal basis for the ETS (anyone wishing a thorough examination of this aspect of the ETS should read Doug Larkin and Paul Badger’s excellent legal paper on the subject), as a matter of common sense and basic logic, if the factual foundation for the OSHA Emergency Temporary Standard is wrong, then the rationale for the ETS is wrong and the ETS itself is wrong—and the factual foundation for the ETS is unquestionably wrong.
Workers are not becoming seriously ill with COVID-19—and certainly not in numbers on par with other workplace injury and illness causes.
Workers are not dying in large numbers from COVID-19.
Workers are most likely contracting COVID-19 at home, not at work.
Workers who have already had COVID-19 are not at danger, grave or otherwise, from reinfection.
Vaccinations do not prevent severe illness and deaths.
The factual and scientific basis for the OSHA Emergency Temporary Standard is wholly demonstrably false. Given OSHA’s legal mandate to ground its decisions in science and not science fiction, this ETS should be withdrawn and never put forward again.