

The Monkeypox Pandemic Panic Has Begun
Corporate Media, Not The Virus, Is The Pox On Our Houses

The WHO is convening a meeting of the very important sounding International Health Regulations Emergency Committee to address the very important question of whether or not the global monkeypox outbreak (was a new name chosen yet?) deserves the very important title of Public Health Emergency of International Concern.
In recent weeks, more than 1,600 monkeypox cases have spread across 39 countries, according to WHO data.
Before this outbreak, monkeypox was only ever seen in areas of central and western Africa. The virus is not thought to be overly dangerous, however pregnant women and children may be at risk.
While no deaths have been reported in newly affected countries, 72 deaths have been recorded from previous outbreaks.
Clearly, this is a very important question.
Current Status Of The Monkeypox Outbreak
As of June 20, there are 2,680 confirmed cases of monkeypox (there’s that stigmatizing name again….will the monkeys ever live this down?) outside of the “endemic” region of Africa where monkeypox is supposed to occur. Outside of Africa, no deaths have been recorded due to monkeypox infection.
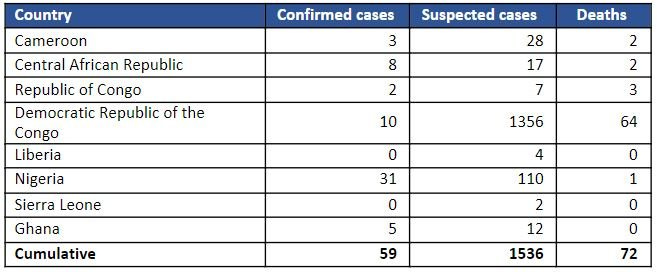
The WHO, for its part, has accomplished another miracle of bureaucratic medicine, by making some 1,536 suspected cases of monkeypox just disappear. In its latest Disease Outbreak News bulletin on monkeypox, the WHO finally decided that the confirmed monkeypox cases in Africa were part of the current “multi-country outbreak” and opted to present the confirmed cases in Africa in the same table as the cases from the other WHO regions.
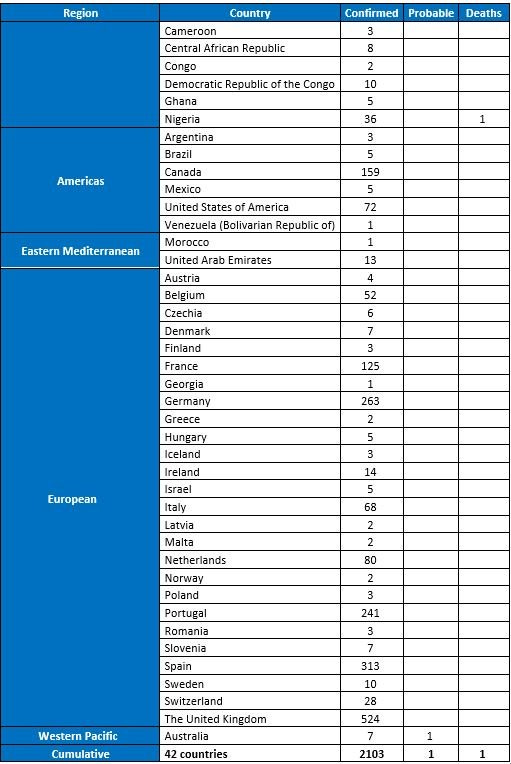
This treatment of the data from Africa, while winning plaudits from the Faucists for its non-stigmatizing fudging presentation of the data, is distinctly at odds with the previous DON bulletin, where the African cases, including the suspected cases, were presented separately.
Apparently, the WHO decided the suspected cases were no longer important.
In previous updates, we included suspected cases and deaths in the African Region. We are now focusing primarily on confirmed and probable cases, including deaths among confirmed and probable cases.
Notch another victory for African virtue-signallers.
In other respects, the non-African cases continue to be reported primarily through sexual health clinics among gay and bisexual men. Buried in the politically correct verbiage of the WHO DON bulletin, however, is the implicit acknowledgment that this has not been the pattern within Africa:
In apparently newly affected countries, cases have mainly, but not exclusively, been confirmed amongst men who self-identify as men who have sex with men, participating in extended sexual networks. Person to person transmission is ongoing, still primarily occurring in one demographic and social group.
Thus the WHO is lumping together two very distinct patterns of transmission into a single outbreak, and pretending there’s no difference between them. Then again, the WHO still hasn’t updated its overview on monkeypox, which it still describes as a “zoonosis” (which the non-African cases clearly are not).
Overall, the WHO rates the public health risk from monkeypox as “moderate”.
Currently, the public health risk at the global level is assessed as moderate considering this is the first time that monkeypox cases and clusters are reported concurrently in many countries in widely disparate WHO geographical areas, balanced against the fact that mortality has remained low in the current outbreak.
The risk to the general public it rates as “low”.
Naturally, it makes sense to declare a low-to-moderate public health risk as an “emergency”. Otherwise, the WHO would just be another clueless bureaucracy spinning its wheels uselessly.
If The Risk Is “Moderate” Why Declare The Virus A Public Health Emergency?
To the skeptic, the WHO’s moderate risk assessment seems at odds with the question of whether or not to declare the virus a Public Health Emergency Of International Concern (PHEIC). Calling monkeypox any sort of “emergency” suggests severe outcomes from monkeypox infection—something a bit beyond fever, aches, and an odd rash in the genital area.
Why is the WHO contemplating a PHEIC declaration for monkeypox?
PHEIC declarations are a part of the International Health Regulations (2005), a global health regulatory framework incorporated by treaty into the health regulations of WHO member states.
Under IHR (2005), a PHEIC is declared by the World Health Organization if the situation meets 2 of 4 criteria:
Is the public health impact of the event serious?
Is the event unusual or unexpected?
Is there a significant risk of international spread?
Is there a significant risk of international travel or trade restrictions?
Given that WHO Director-General Tedros Adhanom Ghebreyesus has already stated the outbreak is “unusual and concerning”, and that international spread is not a “risk” but an established reality, the basic criteria for PHEIC status arguably have already been met.
However, with no deaths outside of Africa, and disease transmission apparently occurring mainly among a single patient demographic, is monkeypox plausibly any sort of “emergency”?
Is the public health impact of 2,680 cases outside of Africa “serious”?
Is there likely to be travel or trade restrictions as a result of the monkeypox outbreak?
Do 2,680 cases outside of Africa truly fit the definition of a PHEIC specified in the IHR (2005)?
“public health emergency of international concern” means an extraordinary event which is determined, as provided in these Regulations:
(i) to constitute a public health risk to other States through the international spread of disease and
(ii) to potentially require a coordinated international response;
Moreover, why is monkeypox an international concern now and not earlier this year, when it was spreading just among the countries of Africa?
Given the WHO’s concerns about “stigma” and “discrimination” over the virus, one has to wonder why spread among Afican countries was not a matter of international concern but spread among European countries is.
Maybe I’m being overly cynical but arbitrarily memory-holing 1500 suspected cases of monkeypox within Africa sounds mighty discriminatory.
We Need More Testing!
In a related vein, the corporate media right on cue is ramping up calls for lots and lots of testing here in the US. The reason we need more testing for monkeypox? Because the UK is reporting more cases—seriously, that’s the rationale of The Washington Post.
Since May 17, when the first case related to a new outbreak was detected on American shores, the United States has identified some 110 cases of monkeypox, a disease caused by a virus similar to smallpox. In contrast, Britain has reported five times as many cases, despite having a population about 20 percent the size. One explanation for this discrepancy could be the relatively larger volume of travel between Britain and countries in which monkeypox is endemic — mainly in western and central Africa. But we strongly suspect another explanation, as well: Britain is doing a far better job of testing than the United States.
Never mind the even more plausible explanation, given the genomic linkage to cases from the 2017 Nigeria outbreak that were “exported” to…wait for it…the UK: Monkeypox is now endemic in Great Britain, and has been for quite some time.
Never mind that even the WHO has noted that the non-African cases of monkeypox are presenting quite differently from what has been the norm for orthopoxviruses: instead of an all-over rash, the European monkeypox cases are display only a few lesions, apparently primarily in the genital region, and in some cases no lesions at all.
Never mind that the Post discredits its own argument for more testing:
We know that monkeypox has gotten ahead of our testing because most monkeypox cases in the United States have not been linked to known infected contacts. If a patient doesn’t know who infected them, that means there is at least one person in the community who is spreading infection to others without knowing it.
If the patient doesn’t know who infected them then more testing is a waste of time—especially since monkeypox appears to be spreading in a manner akin to a sexually transmitted disease.
Even if that were not the case, mass testing for COVID-19 has been a demonstrable failure at achieving any measure of containment. The testing obsession over COVID-19 is hardly an argument for mass testing for any infectious disease.
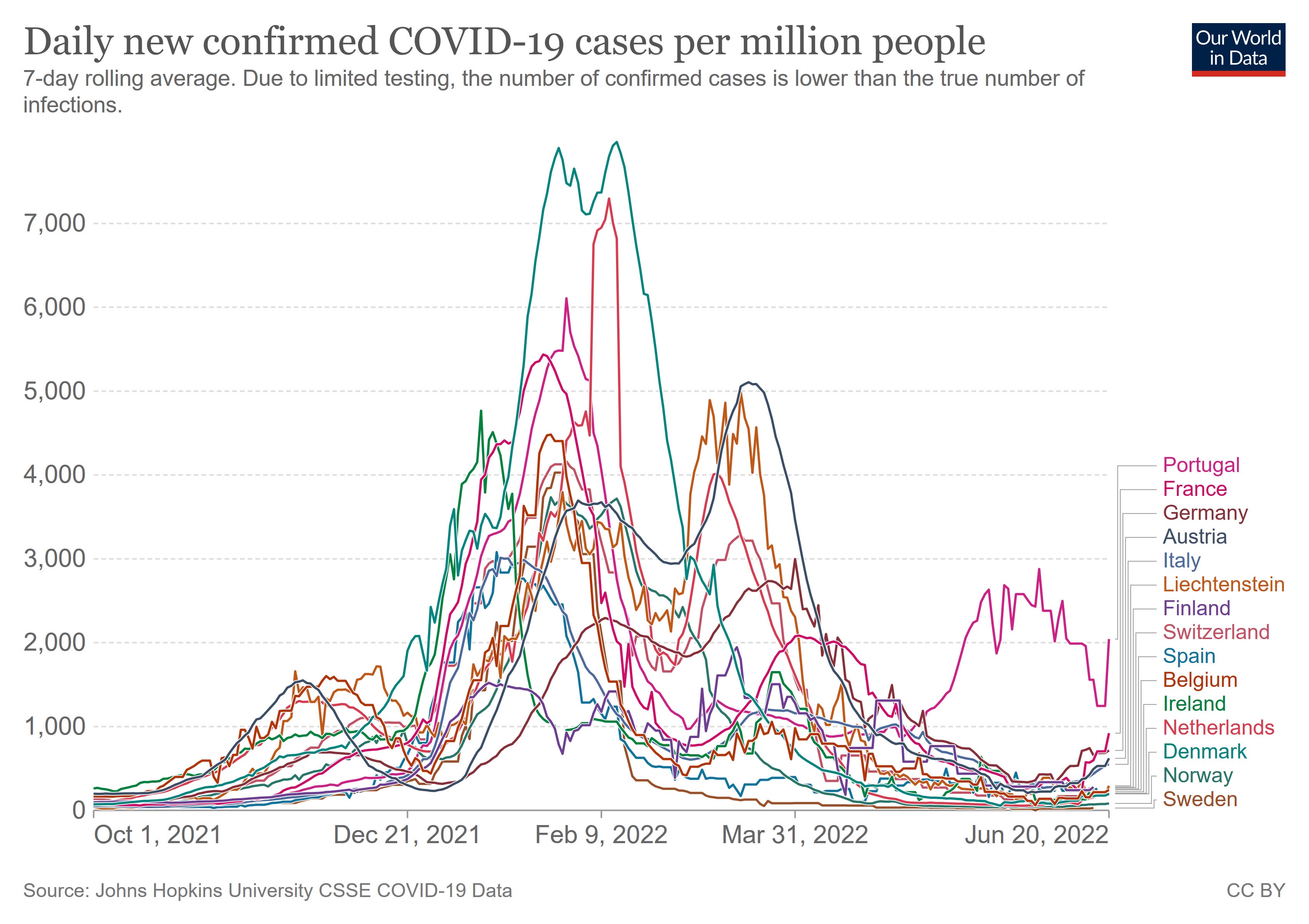
It should also be noted that the daily case counts for monkeypox in any one country do not resemble in the slightest the infection “waves” we see with the SARS-CoV-2 virus.
With monkeypox, the daily case totals are essentially intermittent.
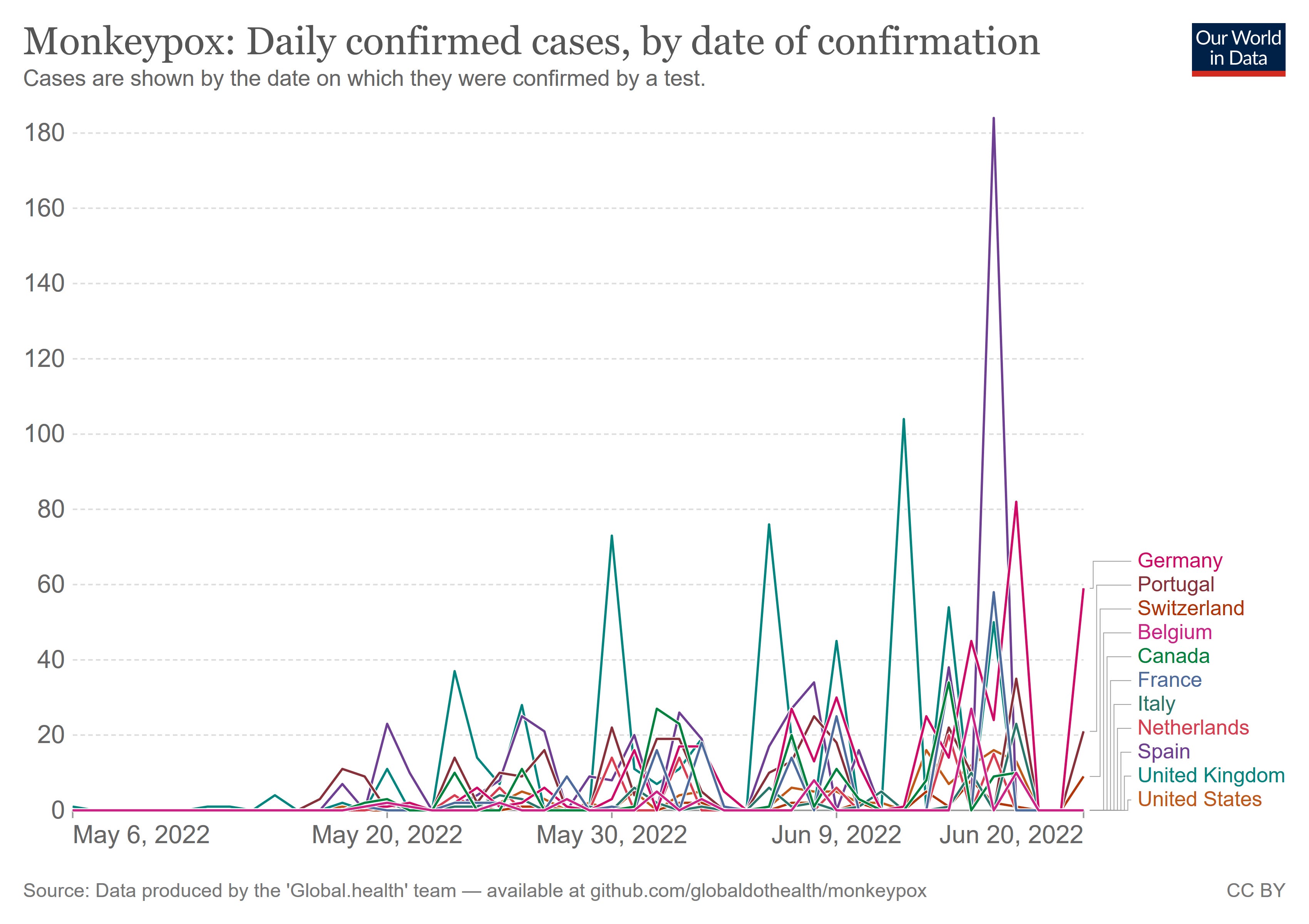
With COVID-19, the cases followed a much more obvious ebb and flow trend.
Regardless of the realities of monkeypox, everyone in the US must be screened regularly for monkeypox, so that we can find every last case of the virus. We mustn’t let Great Britain seize the monkeypox crown uncontested!
Corporate Media Ponders Endemicity
Separately, in The Atlantic we have this lovely bit of pearl-clutching: what if monkeypox finds an animal host species in either North America or Europe which can act as a viral reservoir?
One lasting interspecies hop, akin to the one that SARS-CoV-2 has made into white-tailed deer, and monkeypox will be “with us forever” in the U.S., says Barbara Han, a disease ecologist at the Cary Institute, in New York. In Central and West Africa, where the virus is endemic, scientists suspect that at least a couple of rodent species intermittently slosh it into humans. And as the largest-ever epidemic of monkeypox outside of Africa in history continues to unfurl—more than 2,700 confirmed and suspected cases have been reported across roughly three dozen countries—the virus is now getting plenty more shots on goal. This time, we may not get so lucky; the geography of monkeypox might soon change.
This concern likely comes too late, however. If we accept the premise of “hidden” transmission within Europe and North America—a necessary component of understanding how European cases of monkeypox can have an extraordinary number of nucleotide substitutions—we also have to accept the likelihood that monkeypox has already found an animal host outside of Africa in which to linger when not spreading person-to-person.
Reality Check: Monkeypox Is Not A Pox On Anyone’s House
While there is no denying that the European and North American cases of monkeypox show a dramatic shift the virus’ behavior, evolving from a zoonotic infection to one spread person-to-person, that no one has yet died from this variant is an important perspective on how virulent an infection monkeypox truly is.
Keep in mind that smallpox—the orthopoxvirus that is always lurking in the background of any discussion of monkeypox—had a case fatality rate of approximately 30%. Within Africa, monkeypox itself has a case fatality rate has historically been between 0 and 11%, and more recently has varied from 3 to 6%.
With over 2600 cases confirmed worldwide, this latest manifestation of monkeypox is clearly less lethal than even the West African clade, as a 1% case fatality rate would mean at least 26 fatalities would have occurred by now.
Despite this, and despite the present epidemiological reality of the outbreak being concentrated in a single patient demographic, both the WHO and the corporate media are pushing the rhetoric of crisis and emergency for monkeypox.
We simply must have “international coordination” to stop the spread of the virus.
We simply must have more testing to identify every last case of the disease.
Nothing less than a massive disease control effort spanning the globe and involving mass testing of humanity will suffice for monkeypox.
Or we could simply adopt a simple rule not to canoodle with anyone who has a strange rash anywhere on their body. If someone you know has a rash, just don’t touch it.
The spread of monkeypox outside of Africa is undeniably a noteworthy event. What the spread of monkeypox outside of Africa is not is a crisis, or even a Public Health Emergency Of International Concern. What the spread of monkeypox outside of Africa is not is an emergency of any kind.
Yet you won’t get that message from the corporate media. What you will get instead is a recreation of the Pandemic Panic Narrative for monkeypox. What you will get is a mixture of bad science, poor reporting, and the general promotion of fear, uncertainty, and doubt regarding the virus.
All of which is yet merely more proof that it is the corporate media, and not the monkeypox virus, which is the pox on our houses.
I wonder if The Atlantic knows that one of the first reported outbreaks of monkeypox in the US was because of prairie dogs serving as reservoirs.
I think it's rather interesting how this monkeypox is playing out. I suppose it should remind people to be in-tune with their own bodies and know when things don't look right.
I think if the same recommendations of lockdowns happen, then we'll know what's really going on here. Quite frankly, the mask wearing thing is ridiculous. Of all things, monkeypox should be easy to contain even within a household unlike SARS-COV2. I think the idea of wearing masks around loved ones for fear of them having monkeypox just sounds like something that may have come from the AIDS epidemic of the 1980s.
Maybe Fauci is going back to his roots?
So Monkeypox is not PC. Will scientists, led by Tipper Gore, demand the record label change the title to Major Lance's 'Monkey Time'?
Fun with facts: Quebec has 171 confirmed cases or about 7% of the world's cases. Hmmm. Remember, if you accept that Canada is just about one of the most thoroughly corrupted countries (with Quebec as the supreme leader within its provincial ranks) in the West (as I do). you'd find that statistical anomaly strange. Just talking out loud.