


How fatal is CCPVirus?
Perversely, that is a question the legacy media has never properly answered, nor even attempted to answer. Of all the legacy media's many journalistic sins in covering the CCPVirus "pandemic", their complete ineptitude and even outright dishonesty in addressing the true dangers and risks from the disease unquestionably ranks at or near the top of the list.

We should not be overly surprised, therefore, that close scrutiny of the data reveals the virus to be significantly less lethal than has been claimed in the legacy media. The legacy media has gotten the CCPVirus story wrong from the very beginning, so it perhaps to be expected that they have bungled the most crucial element of the pandemic narrative--the degree to which the virus actually causes fatal disease.
The Data Has Never Reconciled With The Narrative
When considering how badly the topic of fatality has been mishandled by the legacy media, we must remember that the data has never reconciled with the prevailing narrative. As far back as February, I commented on the disparity between the narrative and the number of actual severe cases being observed around the world.
In assembling and digesting the media reports about the COVID-19 coronavirus pandemic (yes, it is a pandemic even though the WHO still dithers and dickers about using the "p-word"), a glaring incongruity stands out: we are missing cases. More precisely, we are missing large numbers of severe cases and pneumonias. Based on the "official" data, there should be far more severe cases reported than there are.
By March, the data made it abundantly clear that, despite the assurances of public health "experts", the lockdown strategies that were implemented in China and Italy failed to contain the disease or alleviate its impacts.
The legacy media has been oblivious to these demonstrable incongruities between the reported data and their preferred narratives, in large part because they have failed to understand the data.
Terminology Matters
Much of the legacy media's misunderstanding of the data can be attributed to a misuse of a single term: "Case Fatality Rate".
As is true of all technical language, Case Fatality Rate has a particular meaning within epidemiology (emphasis mine):
Case fatality rate, also called case fatality risk or case fatality ratio, in epidemiology, the proportion of people who die from a specified disease among all individuals diagnosed with the disease over a certain period of time.
The last part warrants additional discussion. When calculating a Case Fatality Ratio, it is vital to have a reasonably clear assessment of what constitutes an actual "case".
Within the epidemiological context, a "case" is someone who has been diagnosed with a particular disease. As Dr. Malcolm Kendrick explains:
Previously, in the world of infectious diseases, it has been accepted that a ‘case’ represents someone with symptoms, usually severe symptoms, usually severe enough to be admitted to hospital.
A mere positive diagnostic test has not been, historically speaking, sufficient to classify someone as a "case". One has to also be observably and genuinely sick. With CCPVirus, the requirement of being sick has been arbitrarily set aside.
Now, however, we stick a swab up someone’s nose, who feels completely well, or very mildly ill. We find that they have some COVID particles lodged up there, and we call them a case of COVID. Sigh, thud!
A symptomless, or even mildly symptomatic positive swab is not a case. Never, in recorded history, has this been true. Now, however, we have an almost unquestioned acceptance that a positive swab represents a case of COVID. This is then parroted on all the news channels as if it were gospel.
A quick survey of recent reports from around the world suffices to establish the accuracy of Dr. Kendrick's assertions here. Headlines about rising case totals in France and Spain, for example, take little or no notice that, while cases rise, deaths either do not or at a considerably slower rate, as documented by the World Health Organization.
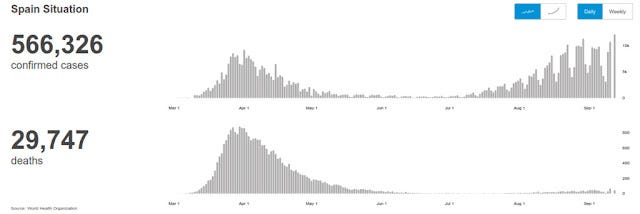
France's recent disease experience has been similar to Spain's: increased cases, no increase in deaths.
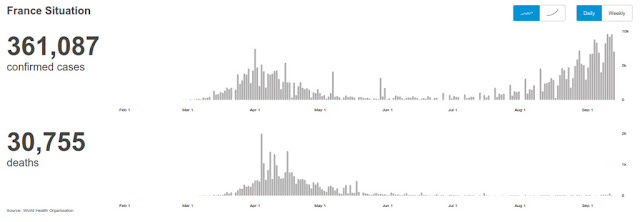
Either the CCPVirus has mutated into a form considerably less lethal than before, or people are being tagged as "cases" who are not really sick.
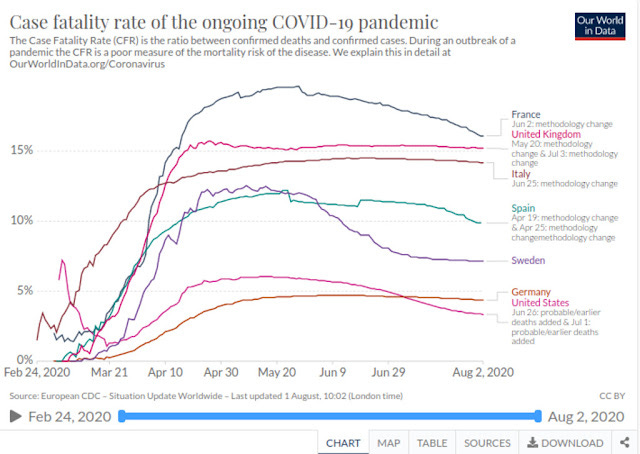
This reality shows up in the United States as well, which sports a lower "Case Fatality Rate" than the most populous countries of Europe, either despite having had a less draconian lockdown than Europe or because of it.
We have further proof that "cases" in the United States include those not genuinely sick from CCPVirus in reports like this from the Miami University, which recently fined students $500 apiece for failing to follow proper guidelines after testing positive for CCPVirus, despite having declining hospitalizations due to the disease at the same time.
If we are counting as "cases" people who are not genuinely sick from CCPVirus, we are misrepresenting the true impact of the disease.
We also run into a similar question mark with respect to what counts as a "CCPVirus death." Per the CDC, only 6% of all recorded CCPVirus deaths had zero co-morbidities, and among the rest there were an average of 2.6 complicating health conditions (diabetes, heart disease, high blood pressure, obesity, et cetera).
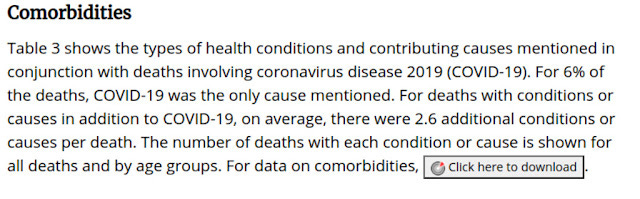
Comorbidities are demonstrably a relevant factor in determining who ends up dying while infected with CCPVirus. With an average of 2.6 "additional conditions or causes" per death with comorbidities, the question invariably arises: did the virus cause the patient to die, or did the additional conditions and causes?
At a minimum, we must acknowledge that people with multiple potentially life threatening conditions are people in relatively frail health, and less able to ward off even minor diseases.
In every scenario, such data by the CDC must lead to a re-evaluataion of even a seemingly obvious term such as "CCPVirus death."
Anthony Fauci Flubbed The Terminology And The Rest Of The World Played Along
Dr. Kendrick goes on to make the case that much of the current conflation and corruption of terminology can be traced to none other than Anthony Fauci, the focal point of so much hue and cry across social media for his commentaries on the CCPVirus "pandemic" in the United States.
Writing in the New England Journal Of Medicine in February of this year, Dr. Fauci made the following observations regarding CCPVirus:
On the basis of a case definition requiring a diagnosis of pneumonia, the currently reported case fatality rate is approximately 2%. In another article in the Journal, Guan et al. report mortality of 1.4% among 1099 patients with laboratory-confirmed Covid-19; these patients had a wide spectrum of disease severity. If one assumes that the number of asymptomatic or minimally symptomatic cases is several times as high as the number of reported cases, the case fatality rate may be considerably less than 1%. This suggests that the overall clinical consequences of Covid-19 may ultimately be more akin to those of a severe seasonal influenza (which has a case fatality rate of approximately 0.1%) or a pandemic influenza (similar to those in 1957 and 1968) rather than a disease similar to SARS or MERS, which have had case fatality rates of 9 to 10% and 36%, respectively.
Buried in this paragraph is a significant terminological error, as Dr. Merrick points out: The CFR for seasonal influenza is 1%, and the Infection Fatality Rate is 0.1%.
It seems that Dr Fauci just got mixed up with the terminology. Because in his Journal article eleven days earlier, he did state… ‘This suggests that the overall clinical consequences of Covid-19 may ultimately be more akin to those of a severe seasonal influenza… [and here is the kicker at the end] (which has a case fatality rate of approximately 0.1%).’
You see, he did say the case fatality rate of influenza was approximately 0.1%. Wrong, wrong, wrong, wrong… wrong.
Oh dear, oh dear, oh dear. With influenza, Dr Fauci, the CDC, his co-authors, the National Institute of Allergy and Infectious Diseases and the National Institutes of Health and the New England Journal of Medicine got case fatality rate and infection fatality rate mixed up with influenza. Easy mistake to make. Could have done it myself. But didn’t.
As the term suggests, the "Infection Fatality Rate" is the ratio of people who die from a disease and all people infected, sick or not.
The infection fatality rate is the measure of how many people who are infected [even those without symptoms, or very mild symptoms] who then die. This is the critical figure to know because it gives you an accurate assessment of the total number of deaths you are likely to see.
The impact of this conflation of terms was compounded by Dr. Fauci's subsequent Congressional testimony:
At a congressional hearing this afternoon, Dr. Anthony Fauci, director of the National Institute of Allergy and Infectious Diseases, suggested that COVID-19 is is considerably more dangerous than run-of-the-mill flu. He observed, "The flu has a mortality rate of 0.1 percent. This has a mortality rate of 10 times that. That's the reason I want to emphasize we have to stay ahead of the game in preventing this."
For whatever reason, whether by accident or design, Dr. Fauci managed to overstate the mortality of CCPVirus relative to seasonal influenza by a factor of ten. By conflating the Case Fatality Rate with the Infection Fatality Rate for seasonal flu, he depicted CCPVirus as being far more lethal when the observed reality is the mortality is on par with the flu.
Significantly, shortly after this, Neil Ferguson of Imperial College in London, released his now-infamous pandemic projection model which forecast 2,200,000 deaths for the United States from the virus. A few weeks later, he would revise his projections downward by more than 90%, amid a growing scandal arising from questions regarding the quality of his model and related computer software (he had himself described the model as "thousands of lines of undocumented C", an enormous red flag to any computer programmer.
As of this writing, the number of recorded deaths in the US from CCPVirus stands at 203,679--somewhat less than 10% of Ferguson's original apocalyptic projection.
Did Neil Ferguson take Anthony Fauci at his word, that CCPVirus was ten times more lethal than seasonal flu, when it is approximately as lethal as seasonal flu? The results certainly lend themselves to that interpretation of events. At a minimum, it seems that Ferguson, Fauci and many others besides all made the same conflation error and wildly overstated CCPVirus mortality.
In other words, the "pandemic potential" of CCPVirus might never have been as great as first feared.
Whither The Crisis?
By greatly expanding the definition of a CCPVirus "case", and by conflating Case Fatality Rate and Infection Fatality Rate during comparisons betwen CCPVirus and seasonal flu, Dr. Fauci and other experts, enabled by an incurious legacy media, depicted a crisis that, by and large, never emerged.
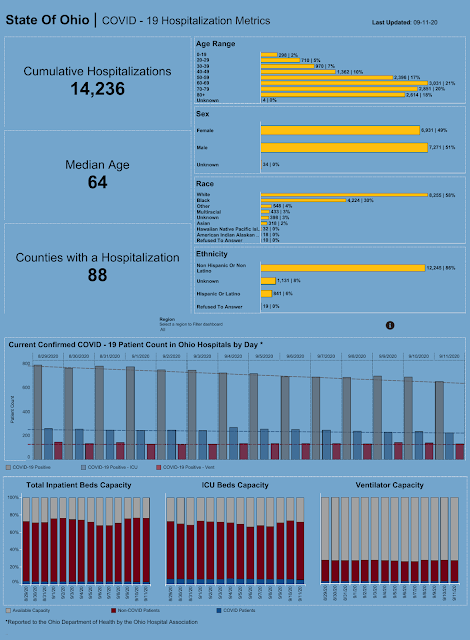
For example, in Harris County, Texas, hospitalizations from CCPVirus were never a majority of hospitalizations, and have never come close to exhausting the available hospital beds.
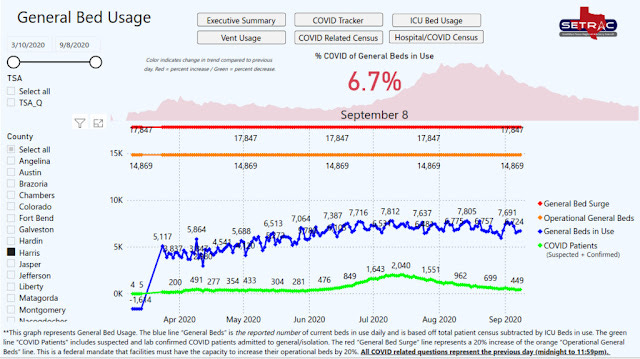
Likewise, Harris County was never faced with a shortage of either pediatric or adult ventilators, nor was the county ever compelled to tap into its "surge" capacity of ICU beds. Regardless of how many cases have been recorded in Harris County, the peak number of hospital cases from CCPVirus stands at 2,040.
Total CCPVirus deaths in Harris County stand as of this writing at 1,658. For perspective, the 2019 population for Harris County, per the United States Census Bureau, is 4,713,325.
In Harris County, at least, there never was a public health crisis due to CCPVirus. It did not happen.
Media Malfeasance
The lack of an actual crisis certainly did not stop the legacy media from reporting as if there were a crisis, even in Harris County. On July 10, 2020, the Texas Tribune ran an article asserting that several Harris County hospitals were experiencing a crush of traffic in their Emergency Rooms due to CCPVirus, and that they were having to turn away patients as a result.
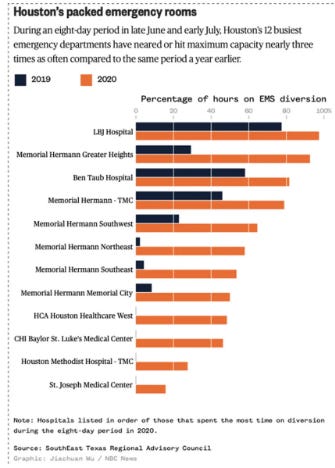
However, there is a significant problem with that reporting: As has already been shown, there was ample bed space in Harris County during the period when the hospital ERs were "overwhelmed."
Why was the available bed space not utilized? Why were patients left to languish in the ER rather than properly admitted to hospital? If patients did not require hospitalization, why could they not be more expeditiously discharged from the ER?
The legacy media has asked none of these questions, and it is unlikely that we will ever see answers to them.
Yet these questions should have been asked. Either hospitals grossly mismanaged their ER resources and denied healthcare to patients as a result, or they simply failed to deliver proper care to CCPVirus patients by not admitting them to hospital in a timely fashion. In any scenario, what was reported by the hospitals to the legacy media--what was regurgitated by the legacy media--was never questioned , even though the extant data did not (and does not still) reconcile to the narrative.
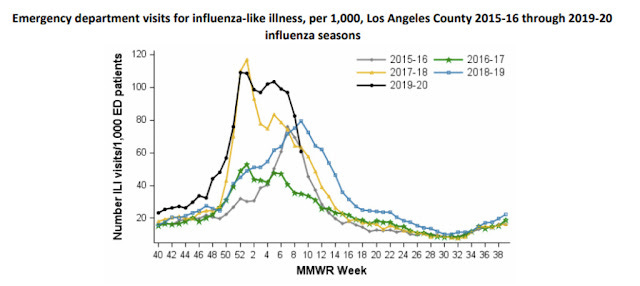
Similarly, when Fox News reported on a UCLA study showing that CCPVirus might have been spreading in Los Angeles back in December, they mis-stated the significance of the observed increase in ER visits for Influenza Like Illness in late December 2019 and January 2020:
This sudden spike in patients with these symptoms, which continued through February, represents an unexpected 50% increase in such cases when compared with the same time period in each of the previous five years.
This is simply not true. Los Angeles'' own InfluenzaWatch reporting for that time frame shows the increase to be greater than the 2018-2019 flu season, as well as the 2015-2017 flu seasons, but it was on par with the 2017-2018 season.
What is also left unremarked is that the UCLA study was the first time any serious attention was given to the increase in ER visits due to ILI symptoms. If the increase in ER visits was due to CCPVirus, then Los Angeles literally had an outbreak of the disease which nobody noticed at the time.
The legacy media narrative plays this off as underscoring the importance of closer scrutiny of patient records.
The findings, the study authors say, demonstrate the importance of analyzing electronic health records to monitor and quickly identify irregular changes in patient populations. The researchers' approach, in which they focused not only on hospitalization data but also on data from outpatient settings, may help epidemiologists and health systems detect future epidemics sooner.
However, the real significance of the story is the lack of media alarm at the time. The late December outbreak (if indeed it was CCPVirus) is in fact the strongest argument to date that the lockdown strategy was simply never needed, at least in Los Angeles. "Business as usual" would have been by far the better approach, because it had already worked once.
As in Harris County, Los Angeles Mayor Eric Garcetti was dealing with a public health crisis that never existed, and that the data shows never existed.
Not Merely Media Malfeasance
It is not merely the legacy media that is guilty of deliberately mis-stating the facts. Emails have emerged which shows the Nashville Mayor's office tried to suppress data which shows that the incidence of CCPVirus cases in the city's bars and restaurants was exceedingly low, with the vast bulk of cases occurring in nursing homes.
Emails between the mayor’s senior advisor and the health department reveal only a partial picture. But what they reveal is disturbing.
The discussion involves the low number of coronavirus cases emerging from bars and restaurants and how to handle that.and most disturbingly how to keep it from the public.
Tennessean reporter Nate Rau succinctly summarized the problem with how Nashville was handling its data:
Tennessean reporter Nate Rau asks “the figure you gave of “more than 80” does lead to a natural question: If there have been over 20,000 positive cases of COVID-19 in Davidson and only 80 or so are traced to restaurants and bars, doesn’t that mean restaurants and bars aren’t a very big problem?
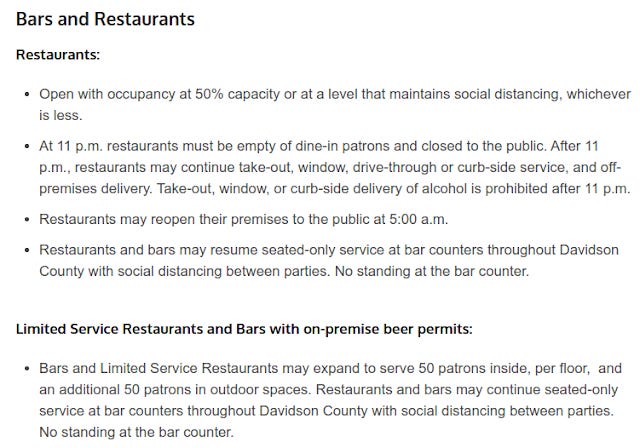
This, of course, cuts to the very heart of the rationale behind lunatic lockdown strategies. If Nashville bars and restaurants only account for 80 CCPVirus cases, why have they been subjected to stringent lockdown guidelines and restrictions? As of this writing, bars are limited to 50 indoor patrons, restaurants are limited to 50% capacity, and all such establishments must close by 11PM:
How does 80 positive CCPVirus tests (not even "cases" as the term has been historically used) justify measures this extreme and more?
Perhaps even more disturbingly, why did the Mayor of Nashville's office elect to suppress specific CCPVirus data sets? It bears noticing that the Nashville Mayor's office has not denied the authenticity of the emails--which is tantamount to an admission they are authentic. Why the coverup?
Again, we weren’t told by the mayor’s office this wasn’t true. We were told to file a freedom of information act request.
Which allows us now to ask the question.why are you keeping this from us? Why would you even want to? Its just the real numbers and what could possibly be an honorable motive?
Nashville, Tennessee, apparently had no public health crisis involving the city's bars and restaurants, but opted to portray the exact opposite to the people through its lockdown orders and "reopening" plans.
The Data Has Always Been Out There
I must emphasize this one point: none of the data I have referenced here comes from any proprietary source. All of it is publicly available, and while I take the precaution of archiving the links to the source material, as proof against subsequent editing or deletion of the linked material, it can all be viewed by following the various links I have provided.
If I can pull in this data via "open source" resources, any reporter for any legacy media outlet can do the same. Only a handful of legacy media reporters have bothered to do so, and even fewer have made meaningful effort to reconcile the data to the narrative.
No one in the legacy media has asked why France is locking down when death rartes are not rising.
No one in the legacy media has asked why Miami University fined students $500 apiece for CCPVirus guidelines when the data shows hospitalizations there decreasing.
The legacy media only belatedly picked up on Nashville's suppression of low case counts from bars and restaurants, which greatly alters the public perception of the outbreak.
No one in the legacy media has exerted any serious effort to hold public health officials accountable, to challenge them on the discrepancies between the data and the narratives being told. No one in the legacy media has made any serious attempt to reconcile the data to the narrative, and address the uncomfortable questions that arise when the data proves to be irreconcilable to the narrative.
No one in the legacy media is attempting to grapple with the fact that our public health officials have so corrupted and conflated essential terms for discussing infectious disease that most any "expert" discussion of CCPVirus is little more than incoherent gobbledygook.
How fatal is CCPVirus? Not very.
No one--almost no one--in the legacy media is willing to give that succinct, honest, straightforward answer to the question.