


After a month of rampant indecision, pearl-clutching, virtue-signalling, and base politicking, Tedros Adhanom Ghebreyesus, World Health Organization Karen-In-Chief Director General, unilaterally decided that monkeypox is seriously really truly a Public Health Emergency Of International Concern. Apparently, almost 16,000 cases beyond Africa with zero deaths1 means it is now officially time for everyone to panic over yet another “novel” viral disease.
Tedros made this decision despite no recommendation from the committee he convened to decide if monkeypox was an emergency.
WHO Director-General Tedros Adhanom Ghebreyesus made the decision on calling monkeypox a global emergency despite a lack of consensus among experts on the U.N. health agency’s emergency committee, saying he acted as “a tiebreaker.” It was the first time a U.N. health agency chief has unilaterally made such a decision without an expert recommendation.
The entire world is now expected to “take monkeypox seriously” because one man (who isn’t even a medical doctor—his doctorate is in “community health”) took it upon himself to declare monkeypox an “emergency”, without the backing of his own emergency committee.
The WHO Director-General is taking the opportunity to express his sincere gratitude to the Chairs and Members of the Committee, as well as to its Advisors, for their careful consideration of the issues regarding this outbreak, as well as for providing invaluable input for his consideration. The Committee Members did not reach a consensus regarding their advice on determination of a Public Health Emergency of International Concern (PHEIC) for this event.
The WHO Director-General recognizes the complexities and uncertainties associated with this public health event. Having considered the views of Committee Members and Advisors as well as other factors in line with the International Health Regulations, the Director-General has determined that the multi-country outbreak of monkeypox constitutes a Public Health Emergency of International Concern.
Yes, that really did just happen.
What Does The Data Say?
What does a Public Health Emergency of International Concern look like? Let’s look at the numbers.
As of 22 July, the US CDC reported 16,836 cases of monkeypox worldwide, with 16,593 cases in countries where the disease is not historically endemic.
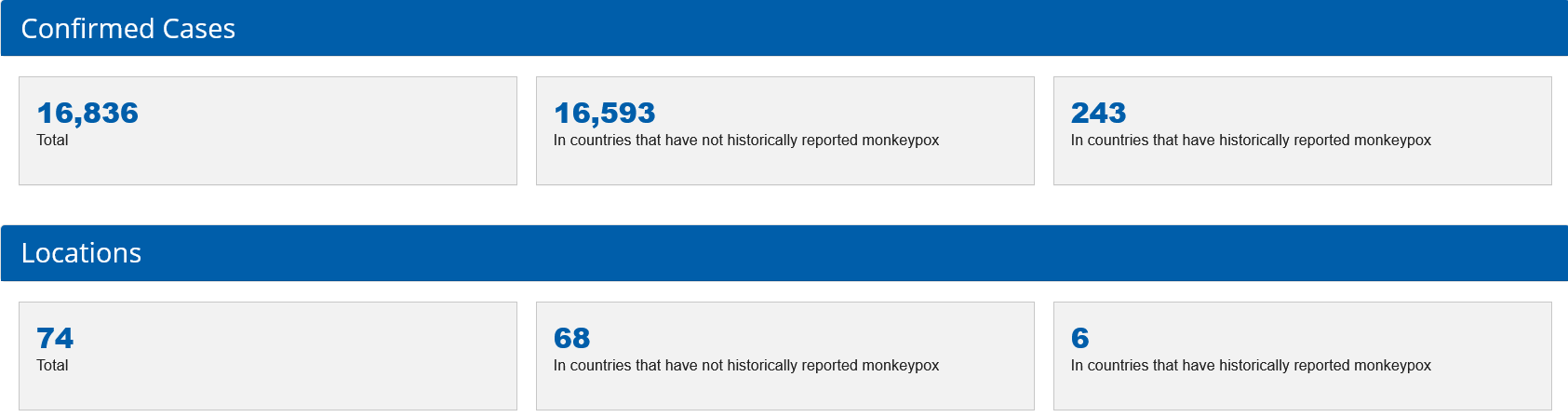
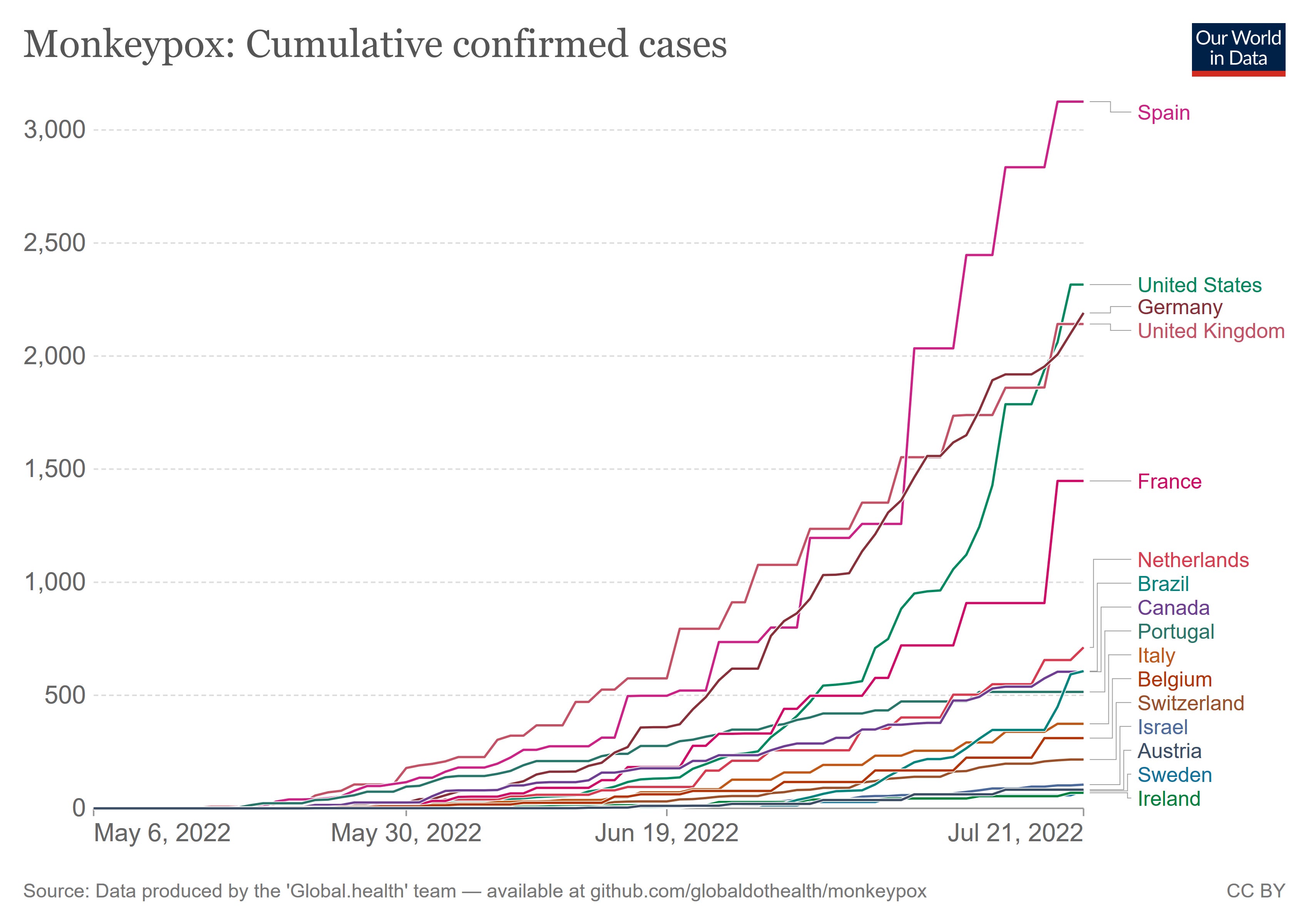
Most of the non-African cases are in Europe. Spain has the most cases, at 3,125. The United States is second with 2,890.2
The virus has two distinct presenatations—one within Africa, where monkeypox is primarily a zoonotic disease, and one beyond Africa, where the virus is primarily transmitted human-to-human.
According to the U.S. Centers for Disease Control and Prevention, more than 16,000 cases of monkeypox have been reported in 74 countries since about May. To date, monkeypox deaths have only been reported in Africa, where a more dangerous version of the virus is spreading, mainly in Nigeria and Congo.
In Africa, monkeypox mainly spreads to people by infected wild animals like rodents in limited outbreaks that typically have not crossed borders. In Europe, North America and elsewhere, however, monkeypox is spreading among people with no links to animals or recent travel to Africa.
WHO’s top monkeypox expert, Dr. Rosamund Lewis, said this week that 99% of all the monkeypox cases beyond Africa were in men and that of those, 98% involved men who have sex with men. Experts suspect the monkeypox outbreaks in Europe and North America were spread via sex at two raves in Belgium and Spain.
To summarize, there are two distinct types of monkeypox in circulation. One is primariliy in Africa and occasionally lethal. One is spread outside of Africa and has killed no one. The strain/clade/variant outside of Africa is almost entirely being spread among gay and bisexual men.
Aside from the 16,000+ cases, does this sound like the sort of disease that is a public health emergency at either a local, national, or international level? You tell me. The WHO Director General on his own initiative has said this does look exactly like a public health emergency, and at an international level at that.
It is somewhat ironic that when monkeypox was spreading just within West and Central Africa, and causing as many as 72 deaths, Tedros, who is Eritrean, did not think it was an emergency then, but a disease outside of Africa which has yet to kill anyone is unquestionably an emergency. Draw your own conclusions.
Not One Outbreak, But Two
As I had noted at the beginning of June, the significant differences in how monkeypox is presenting in West and Central Africa, and how it is presenting outside of Africa, is a strong signal that these are two significantly different strains of monkeypox, with radically different characteristics regarding transmissibility and pathogenecity. Not only is this a grim confirmation that the virus has undergone significant mutation and evolution, but that the disease is now entrenched and endemic within at least Europe.

It is emblematic of the functional lack of seriousness of Fauscists everywhere that they are more worried about the name of the virus somehow stigmatizing and demeaning those who may not even be impacted by the new strain than they are about the emergence of a new strain with radically different behavior. Yet in their open letter last month detailing how monkeypox should be renamed and why, they presented genomic evidence for their proposed new taxonomy for monkeypox which goes a long way towards confirming that the strain spreading outside of Africa is indeed a new strain significantly different from the West African strain from which it evolved—and completely missed the epidemiological significance. Even the WHO has managed to not notice the vast differences in behavior between the new strain and its ancestor.
Yet with 16,000 cases outside of Africa, vs less than 1,000 “official” cases in Africa, and zero deaths outside of Africa vs five official deaths in Africa, the epidemiological evidence alone shows that this is not a singular outbreak of disease, but rather two: traditional monkeypox, which is still primarily zoonotic and spreads largely from animal to human, and “new monkeypox”, which may not be truly zoonotic and is being spread almost exclusively human to human. Biologically and genetically, the two strains are still monkeypox, but the newer strain is proving itself to be an extreme divergence from its parent lineage, even to the extent of having a potential endemic region (Europe) that is wholly outside of Africa itself.
The WHO has chosen to ignore the evidence that was plain even a month ago, and is largely ignoring the African outbreak of traditional monkeypox as a result.
Is New Monkeypox An STD?
One question which is relevant about the new strain is whether or not it should be considered a form of sexually transmitted disease. At first glance, the case for counting it as an STD seems fairly strong: the primary vector for transmitting the disease appears to be sexual activity among gay and bisexual men, and clinical research backs this up.
We report 528 infections diagnosed between April 27 and June 24, 2022, at 43 sites in 16 countries. Overall, 98% of the persons with infection were gay or bisexual men, 75% were White, and 41% had human immunodeficiency virus infection; the median age was 38 years.
However, there is also an important caveat: based on what is known about the actual transmission, the primary requirement is close skin-to-skin contact with an infected individual, not necessarily sexual acts themselves.
“Monkeypox is not a sexually transmitted disease in the classic sense (by which it’s spread in the semen or vaginal fluids), but it is spread by close physical contact with lesions,” Northwestern Medicine infectious diseases expert Robert L. Murphy, MD, said last month in a Northwestern University news release.
It is this skin-to-skin requirement that has led the CDC to issue guidance to “have sex with clothes on” as a way to minimize the spread of the virus by covering up monkeypox lesions—because during an emergency people still need to have sex, apparently.
Even the WHO’s emergency committee meeting has noted the sexual element of the global transmission. Not only are a majority of cases being spread by sexual activity among gay and bisexual men, in the US and Canada upwards of 99% of all cases involve gay and bisexual men, whereas the Nigerian cases of traditional outbreak apparently do not.
In the United States, cases of monkeypox are widely distributed across the country, although most cases are concentrated in three large cities. While a few cases have occurred in children and a pregnant woman, 99% are related to male-to-male sexual contact.
In Canada, 99% of cases have occurred among MSM, and the country is taking a broad approach to pre-exposure prophylaxis, given the challenges with contact tracing; and is strongly focused on engagement with community-led organizations supporting key affected populations groups.
Nigeria recorded a little over 800 cases of monkeypox between September 2017 and 10 July 2022 and has seen at 3% case fatality ratio among confirmed cases. Cases are predominantly in men aged 31 to 40 years; there was no evidence of sexual transmission presented. The highest number of annually reported cases since 2017 has been observed in 2022.
To be clear, this does not make new monkeypox a “gay disease.” Viruses don’t give a damn about sexual orientation, and, for the record, neither do I. Sexual activity is not the only means of spreading the disease, although it is at this time by far the most common means—it’s not “gay sex” that is at issue but promiscuous sex, as the recent study also documents:
The suspected means of monkeypox virus transmission as reported by the clinician was sexual close contact in 95% of the persons. It was not possible to confirm sexual transmission. A sexual history was recorded in 406 of 528 persons; among these 406 persons, the median number of sex partners in the previous 3 months was 5 partners, 147 (28%) reported travel abroad in the month before diagnosis, and 103 (20%) had attended large gatherings (>30 persons), such as Pride events. Overall, 169 (32%) were known to have visited sex-on-site venues within the previous month, and 106 (20%) reported engaging in “chemsex” (i.e., sex associated with drugs such as mephedrone and crystal methamphetamine) in the same period.
Call me old fashioned but maybe the message here should be that attending drug-fueled orgies are not the way to stay safe and healthy?
Let The Virtue-Signalling Begin
Of course, the utility of such pedestrian health control measures as self-restraint are of no importance to the virtue-signallers in the media, who have not wasted any time in denouncing the US response to the global outbreak, claiming the US is “failing” to respond adequately to the disease.
On Saturday, Dr. Tedros Adhanom Ghebreyesus, director-general of the World Health Organization, declared that monkeypox is a public health emergency of international concern, despite a special WHO committee being unable to reach consensus. That kind of indecisiveness represents much of the monkeypox response so far. With more than 2,800 cases and counting, the U.S. is already failing at its monkeypox response, and without urgent efforts, the virus could establish itself permanently.
Naturally, the virtue signallers want everyone vaccinated against monkeypox, not just the ones who are actually catching and spreading it—through, it must be acknowledged, activity that is both voluntary and avoidable.
“It’s clear that we’re going in the wrong direction,” said Gregg Gonsalves, an epidemiologist at Yale School of Public Health. “We could have treated this like an emergency, both globally and domestically, in May… It should be all-hands-on-deck.” In order to curtail the outbreak, officials need to focus urgently on diagnosing and preventing cases in the communities and close contacts of those at most risk.
The one serious point that has emerged in the virtue-signalling is the potential for the disease to find new transmission vectors, including spreading in areas such as gyms and day-care facilities. With close contact with monkeypox lesions, or even just the fluids from such lesions, being the apparent actual mode of transmission, it cannot be denied that there is nothing readily apparent about the disease which limits it to a particular patient demographic.
However, that risk also must address the question: why has that not yet happened? So far in the US, only two children have been confirmed to have monkeypox, and both appear to be in close proximity with individuals in the current affected demographic. Spread through child daycare has not yet been documented, nor has spread through a gym or similar facility. Gay and bisexual men do have families, do put their children in daycare, and do work out at gyms, so even if the primary transmission vector is a sexual one, the potentials for transmission into other areas by other vectors have always been present—and have not, for whatever reason, been realized.
This is not to say that such potentials won’t be realized—the cases involving children already disprove that notion—but that understanding why such potentials are slow to being realized very likely would shed some important light on why the disease is spreading so quickly among the current patient demographic.
Such practical thinking, of course, matters not to the virtue-signallers. Panic and hysteria are, after all, so much more emotionally gratifying. There’s no porn like fear porn.
Monkeypox Is A Concern, Not A Crisis, Not An Emergency
Globally, monkeypox is undeniably a health concern. Any disease that can spread globally and erupt as rapidly as monkeypox appears to have done should be taken seriously. Prudent responses are warranted.
Yet prudent response means realistic response. Massive doses of vaccine are not going to be immediately available for the simple reason that there is no actual monkeypox vaccine, nor even any actual monkeypox antiviral therapy. The vaccines and treatments that exist are for smallpox, and are presumed to be effective against monkeypox, although the actual data on this point is limited at best. Non-pharmaceutical interventions are going to be the most impactful—and likely will even after the vaccines and therapeutics become more widely available.
Non-pharmaceutical interventions at this point means, of course, attention to good hygiene and cleanliness, taking care to minimize contact with the clothing and bedding used by infected individuals. Refraining from frequent and largely anonymous sexual encounters, “stigmatizing” and “discriminatory” as that may be, is almost sure to be the best way to avoid getting infected, and abstaining from sex while infected is unquestionably the best means to prevent transmission.
Which makes this current outbreak an utter absurdity: if consensual sex is the primary transmission vector, this outbreak could be stopped today simply by a temporary period of sexual abstinence. This outbreak need never have happened in the first place, which alone makes it qualitatively different from COVID-19 or other large outbreak of disease.
Contrary to the posturings of the WHO Director General, monkeypox is at most a global health concern. It is not a crisis and it is certainly not an emergency. It is not a call for new mass vaccination campaigns, and it would be an ethical abomination to misuse monkeypox as a cheap excuse to pump more injections in to more arms.
The global monkeypox outbreak is a call not for “all hands on deck”, but for a few more cold showers and a little less impulse gratification. Self restraint remains the best viral self defense on the planet.
No one has died from or with monkeypox outside of Africa. Officially, the WHO only acknowledges five deaths within Africa, although in the Disease Outbreak News Bulletin of 10 June, the WHO acknowledged 72 deaths in Africa among “suspected” monkeypox cases. In the subsequent DON Bulletin of 17 June, the WHO dropped the suspected cases and only reported the confirmed cases, dropping the number of deaths to just 1. By the second meeting of the WHO’s IHR Emergency Committee on 21 July, the WHO acknowledged 5 deaths, all in Africa (3 in Nigeria and 2 in the Central African Republic). That total really should be 75, including the 71 suspected deaths the WHO decided to memory-hole last month.
Our World In Data cuts off a day earlier than the CDC report, and so the graph has lower totals. The patterns of case rises, however, is the same.
Oh, but that's exactly what they want: More jabs. Canada, the USA, Germany and UK all ordered MILLIONS of vaccines. Try and tell me, the four main countries at the centre of the Corona scandal-scam, this is not a money grab or what they call 'moneypox'.
They're using the exact same playbook from Covid to drum up fear. Notice the use of 'novel' again. And where the fear (read lie) of asymptomatic spread managed to induce hysteria, 'atypical' is the description I've heard used by The Experts (TM).
The preventative Mother Kar-Hens are out in full force. The epidemiologists are getting a second round of 15 minutes. Lucky them.
Chalk another one up for the conspiracy theorists because they warned about this (and Marburg) last year. In fact, they warned the objective was permanent pandemics in 2020.
Here we are.
Declaring health emergencies for 16 000 people and no deaths.
Don't even bother trying to pretend there aren't crimes against humanity in play.
"it’s not gay sex that is at issue but promiscuous sex"
Sure, but what demographic is by far the most promiscuous?