


Apparently, not enough people have died from COVID-19, according to USA Today.
More precisely, the number of COVID-19 deaths and estimates of excess mortality in the US are not lining up cleanly, with some 200,000 “excess” deaths not attributed to the pandemic that should be.
Nationwide, nearly 1 million more Americans have died in 2020 and 2021 than in normal, pre-pandemic years, but about 800,000 deaths have been officially attributed to COVID-19, according to the CDC data. A majority of those additional 195,000 deaths are unidentified COVID-19 cases, public health experts have long suggested, pointing to the unusual increase in deaths from natural causes.
Put simply, most, if not all, excess death since the beginning of 2020 “must” be due to COVID-19. It is inconceivable for there to be any alternative—at least, if one follows and accepts the media's pandemic panic narrative.
Yet if one looks at the data, there is at least a possibility the exact opposite is true—that rather than not having counted enough COVID-19 deaths, we quite possibly are overcounting them.
Know Thy Symptoms
The story would be more credible if the authors accurately presented the panoply of co-morbid conditions. At the very least they should avoid cringeworthy statements like this one:
Instead, they list conditions with symptoms that look a lot like COVID-19, such as Alzheimer’s disease, hypertension and diabetes.
Chew on that for a moment. COVID-19 presumably looks a lot like Alzheimer's disease, hypertension, and diabetes.
Oh really?
These are the symptoms of COVID-19 per the CDC:
People with COVID-19 have had a wide range of symptoms reported – ranging from mild symptoms to severe illness. Symptoms may appear 2-14 days after exposure to the virus. Anyone can have mild to severe symptoms. People with these symptoms may have COVID-19:
Fever or chills
Cough
Shortness of breath or difficulty breathing
Fatigue
Muscle or body aches
Headache
New loss of taste or smell
Sore throat
Congestion or runny nose
Nausea or vomiting
Diarrhea
This list does not include all possible symptoms. CDC will continue to update this list as we learn more about COVID-19. Older adults and people who have severe underlying medical conditions like heart or lung disease or diabetes seem to be at higher risk for developing more serious complications from COVID-19 illness.
For comparison, these are the symptoms of mild Alzheimer's Disease per the National Institutes of Health:
In mild Alzheimer’s disease, a person may seem to be healthy but has more and more trouble making sense of the world around him or her. The realization that something is wrong often comes gradually to the person and his or her family. Problems can include:
Memory loss
Poor judgment leading to bad decisions
Loss of spontaneity and sense of initiative
Taking longer to complete normal daily tasks
Repeating questions
Trouble handling money and paying bills
Wandering and getting lost
Losing things or misplacing them in odd places
Mood and personality changes
Increased anxiety and/or aggression
Alzheimer’s disease is often diagnosed at this stage.
According to the CDC, hypertension (high blood pressure) has no real symptoms:
High blood pressure usually has no warning signs or symptoms, and many people do not know they have it. Measuring your blood pressure is the only way to know whether you have high blood pressure.
Finally, these are the symptoms of diabetes, also per the CDC:
If you have any of the following diabetes symptoms, see your doctor about getting your blood sugar tested:
Urinate (pee) a lot, often at night
Are very thirsty
Lose weight without trying
Are very hungry
Have blurry vision
Have numb or tingling hands or feet
Feel very tired
Have very dry skin
Have sores that heal slowly
Have more infections than usual
Do these three conditions sound even remotely similar? Is it really plausible that a medical doctor would unable to distinguish one from the others? To both questions, the answer is a clear and unambiguous “No'“.
COVID-19 is not Alzheimer’s, hypertension, or diabetes, and beware the healthcare professional unable to make the distinction. There are still non-COVID diseases still making an impact.
Where Are The Excess Deaths?
Just as all disease is not COVID-19, not all excess deaths in the past two years are attributable to COVID-19. People still die from causes besides the SARS-CoV-2 virus.
Moreover, when we examine the CDC estimates of excess death for various causes, respiratory ailments—where one would expect excess death from COVID-19 (a respiratory illness by definition) to appear—show very little excess death over the past two years.
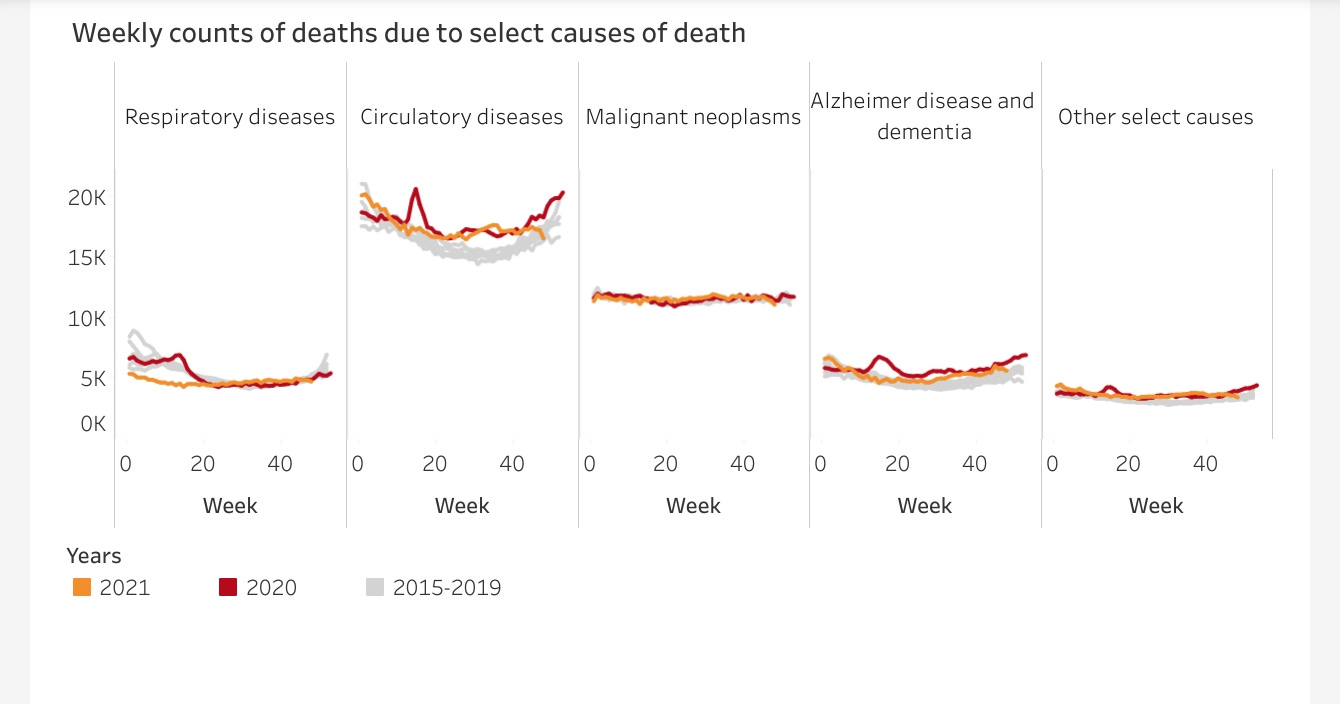
Indeed, for the first part of 2021, there were fewer deaths due respiratory illnesses than the 2015-2019 historical average. At a time when COVID-19 was peaking in the US, there was no excess death from respiratory illnesses. There was, however, excess death from circulatory diseases for most of both 2020 and 2021. The same is true for Alzheimer’s.
Drilling into each of these disease categories we find, indeed, the pandemic infectious respiratory disease has produced little excess death from any sort of respiratory disease.
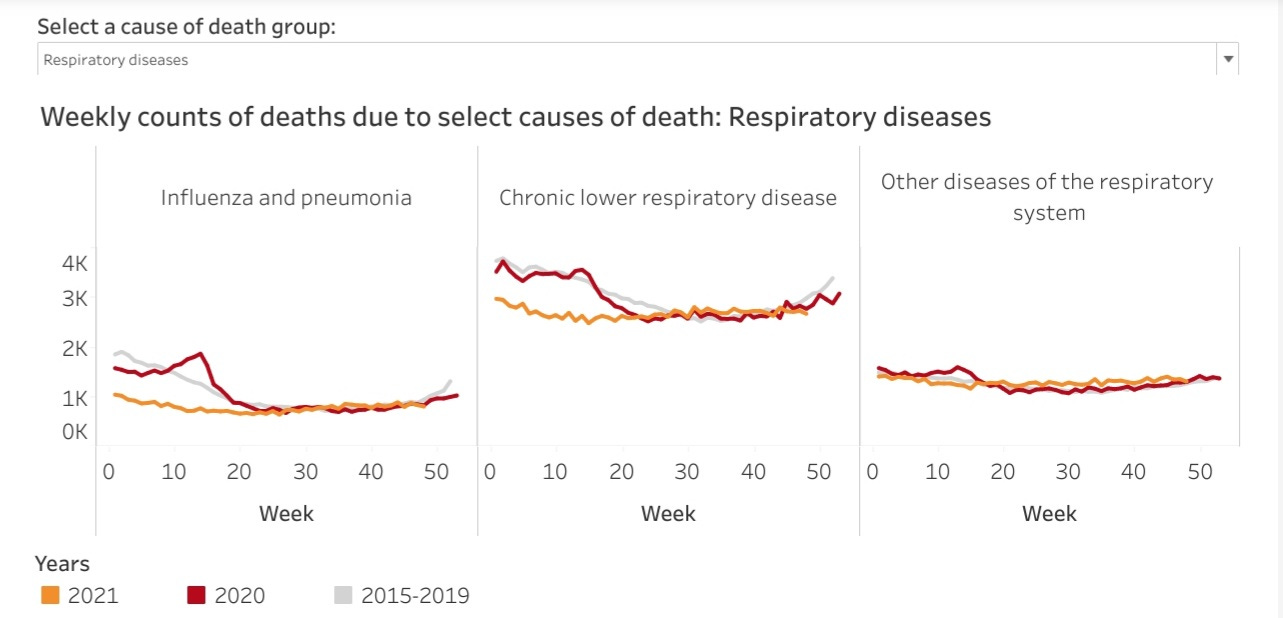
Even though research establishes the SARS-CoV-2 virus as a respiratory infection, with the lungs as the primary target, but for a brief spike in 2020, the excess mortality data shows little or no excess death from pneumonia, lower respiratory infections, or any respiratory illness.
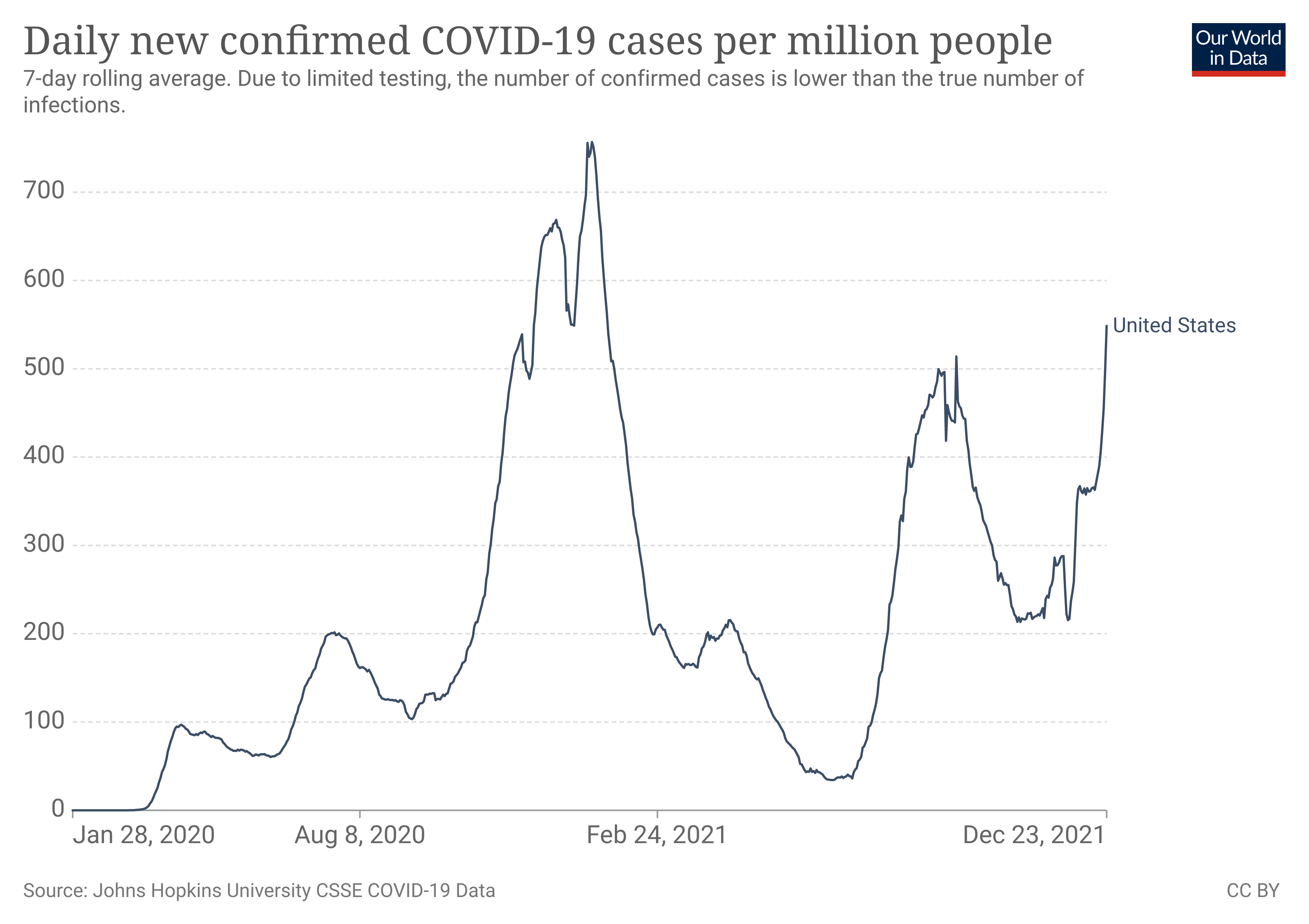
Even more intriguingly, the CDC data shows no spike in deaths from respiratory illnesses in the early weeks of 2021, a time when the data shows COVID-19 was peaking.
If people are dying from and with COVID-19, those deaths from a respiratory disease are not appearing as excess deaths from respiratory disease, per the CDC data. To call this ”counterintuitive” is something of an understatement.
Contrary to what USA Today proposes, if anything COVID-19 deaths arguably are over counted, not undercounted. Alternatively, the mainstream assessment of COVID-19 and its disease trajectory is either incomplete or inaccurate.
Too Many Heart Attacks And Strokes
Where we do see excess death during the pandemic era is in ischemic heart and hypertensive diseases.
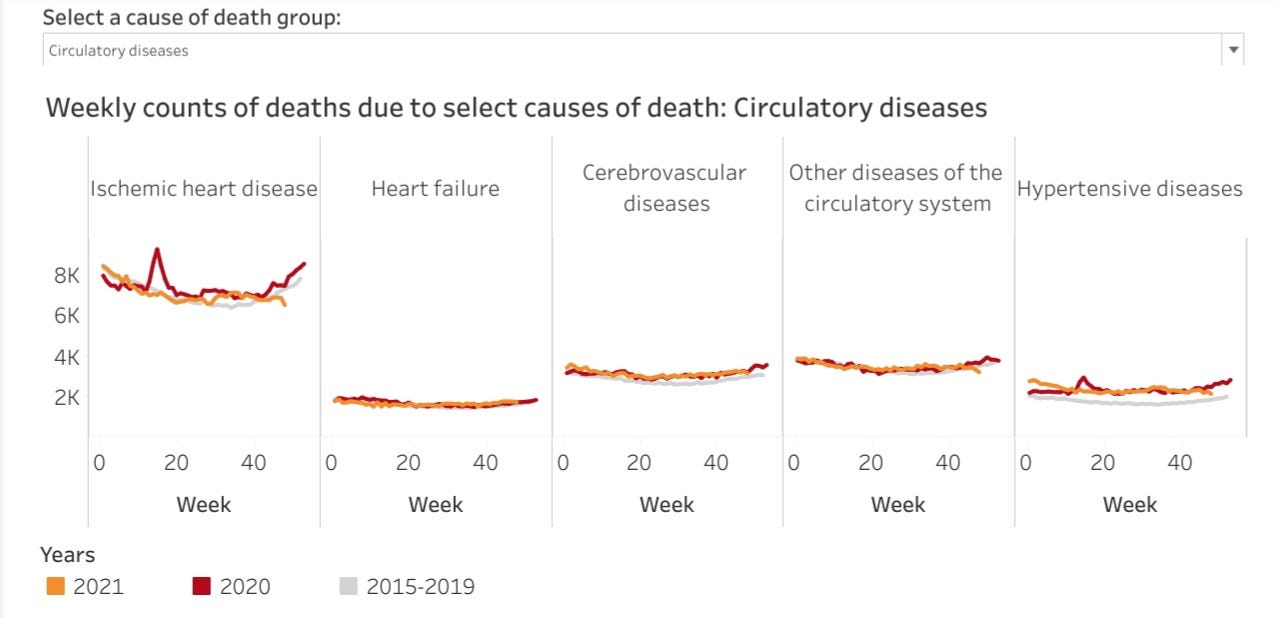
The way that COVID-19 kills, according to the data, is through heart attacks and strokes. Whether that makes COVID-19 a cardiac ailment is a debate I shall leave to the virologists and cardiologists. For now, it is sufficient to note that COVID-19, considered a respiratory disease, appears to present greater mortality risk from cardiac and circulatory illness than from respiratory illness.
However, even within the data on circulatory disease death, we see no spike of excess death during early 2021, at a time when there was a significant reported spike in COVID-19 deaths.
No matter how COVID-19 works to extinguish human life, we should see the early 2021 surge in COVID-19 deaths reflected in the CDC mortality data. All reported deaths are placed in one category or another, so regardless of the particular mechanism of death, we should see mortality and excess death variances broadly coincide with COVID-19 cases and deaths, and we do not.
Ultimately we are presented with the same uncomfortable question: are COVID-19 deaths being over-counted?
All Deaths Matter
Let us be clear on this much: death is death, and it is unseemly haggle overmuch whether someone died “with COVID-19”, “from COVID-19” or from some other cause entirely. Where people have died, common decency says we should give proper space for grief and mourning.
Yet neither should we disregard the many causes of death. In particular we must scrutinize how an infectious respiratory disease such as COVID-19 can produce death. Such details are essential both in establishing effective public health policies regarding COVID-19 and in individuals establishing for themselves their particular risk mitigation strategies.
Most of all, neither the media nor the “experts" should be seeking to magnify COVID-19 mortality when their own “official” data sets show a significant probability that COVID-19 mortality is already being overstated.
Outstanding summary, Peter. You've, once again, included the variables the PTB/media should have.