


"Science", we are told, is the foundation of all which the Centers for Disease Control (CDC)—the government agency tasked with protecting the nation's public health—undertakes. Their decisions and recommendations are always guided by science—and presumably not by politics.
How do we know this? They tell us this. They promise us this.

From the CDC's "Pledge To The American People":
Base all public health decisions on the highest quality scientific data that is derived openly and objectively
When it comes to the current COVID-19 (aka "CCPVirus") pandemic, however, they are falling far short of the mark. Many of their decisions and pronouncements lack scientific support or scientific rigor. The latest and most glaring example of this is the hype du jour over the wearing of masks and facial coverings to mitigate the spread of the disease.
In The Beginning, Masks Were Bad
At the beginning of March, the US Surgeon General Dr. Jerome Adams was quite emphatic: wearing a mask could increase your risk of contracting CCPVirus.
"You can increase your risk of getting it by wearing a mask if you are not a health care provider," Adams said during an interview on Fox & Friends on Monday morning.
"Folks who don't know how to wear them properly tend to touch their faces a lot and actually can increase the spread of coronavirus," Adams said.
Even as late as March 30, the World Health Organization (WHO) advised against wearing masks.
"There is no specific evidence to suggest that the wearing of masks by the mass population has any potential benefit. In fact, there's some evidence to suggest the opposite in the misuse of wearing a mask properly or fitting it properly," WHO executive director of health emergencies Mike Ryan said Monday.
The legacy media had been advocating the "no mask" position quite strongly even before March.
Even if there are cases next door, the answer is no, you do NOT need to get or wear any face masks—surgical masks, "N95 masks," respirator masks, or anything else—to protect yourself against the coronavirus. Not only do you not need them, you shouldn’t wear them, according to infection prevention specialist Eli Perencevich, MD, a professor of medicine and epidemiology at the University of Iowa’s College of Medicine.
"The average healthy person does not need to have a mask, and they shouldn’t be wearing masks," Dr. Perencevich said. "There’s no evidence that wearing masks on healthy people will protect them. They wear them incorrectly, and they can increase the risk of infection because they’re touching their face more often."
The message was clear: masks were bad. Do not wear masks.
In The Beginning, There Was Science
This position is the position that is actually supported by science. There is no evidence that a community strategy of wearing masks or facial coverings has any effect in containing infectious disease.
There are at least four separate studies on the effect of healthy people wearing masks as well as hand hygiene around symptomatic individuals:
There is the 2008 Hong Kong study of 198 households, which found "The laboratory-based or clinical secondary attack ratios did not significantly differ across the intervention arms." In other words, the masks made no difference.
There is the 2009 Australian study of 286 individuals across 143 households which concluded that "...household use of face masks is associated with low adherence and is ineffective for controlling seasonal respiratory disease."
There is the 2009 Hong Kong study of 259 households which found that among the mask-wearing groups "the differences compared with the control group were not significant."
There is the 2012 German study of 84 households comparing mask-only (M) and mask-plus-hand-hygiene (MH) strategies which found "there was no statistically significant effect of the M and MH interventions on secondary infections."
One point must be emphasized: these studies evaluate wearing masks as a mitigation/containment strategy. These studies do not offer any insight or commentary on the efficacy of an individual mask at blocking individual virion particles from entering the nose and mouth.
The scientific evidence, therefore, aligns with the statements by the US Surgeon General, the WHO executive director, as well as various doctors consulted by the legacy media. There is no scientific basis for any argument that a community strategy of wearing masks has appreciable impact on disease spread.
As for the assertions of risks associated with wearing masks, a 2019 study of 59 healthcare workers in Illinois found significant contamination on the outside of protective gear, and even on the individual's bare skin. Similar findings resulted in another 2019 study of 148 healthcare workers in Beijing. Self-infection during the removal of a contaminated mask unquestionably is a risk associated with wearing a mask. Dr. Adams' assertion that people could place themselves at greater risk of CCPVirus infection was therefore also supported by scientific evidence.
Narrative Change: Masks Are Good
At the end of March, the legacy media narrative shifted and began to advocate for the general wearing of masks. Much of the driving force for the change appears to have been public sentiment regarding masks.
The national discussion about mask-wearing has since become more ambiguous. The public health advice remains the same, but critics say the guidance was wrong and confusing and may have encouraged mask-hoarding.
There's a #masks4all movement on social media that argues for universal mask-wearing amid the pandemic, with some proponents saying it shows community solidarity in the fight against coronavirus.
Additionally, academics such as Harlan Krumholz, Professor of Medicine at Yale University, came out strongly in favor of "universal precautions" strategy for healthcare workers.
The infection of health-care workers (and patients by health-care workers) should be understood as a safety issue — that is, preventable with proper, high-quality practices. We should commit to making it a "never event. As a result, harm to a health-care worker, and by extension, to their families and friends as a result of their service on the front lines, should be a never event. It seems within our grasp to make it so.
Professor Krumholz extended his advocacy, however, beyond healthcare workers to include all manner of first responders, but also store clerks and retail staffs.
And we should be thinking of this more broadly as extending to everyone providing vital services on the front lines, including police officers, firefighters, cashiers at pharmacies and grocery stores, and others in such positions. All of these individuals are placing themselves in the path of the virus to help others. Yet, they can infect and be infected. We need not only the PPE but also the mind-set.
As far as healthcare workers are concerned, Professor Krumholz' advocacy is backed up by scientific data. A 2011 study of 1,411 healthcare workers in 15 Beijing hospitals confirmed that wearing either surgical or N95 masks resulted in statistically significant lower rates of infection among healthcare workers. However, overall infection rates even among non-mask-wearing healthcare workers was only 9%, making extrapolation to the broader categories of first responders and retail workers problematic at best, particularly in light of the other four studies cited earlier.
In arguing for extending the mask protocol to other categories of workers, Professor Krumholz would appear to be stretching the science somewhat.
This is also where Professor Krumholz engages in a bit of fallacious reasoning. By claiming that "we know with reasonable confidence that personal protective equipment, commonly known as PPE, can decrease risk," he is guilty of a faulty generalization (also known as a "hasty generalization"). As the foregoing studies demonstrate, while there are sound arguments for PPE among healthcare workers, PPE does not provide the absolute measures of protection he quite reasonably desires for healthcare workers, and the efficacy of PPE for non-healthcare workers is in fact problematic.
The legacy media, true to its infotainment form, has never delved meaningfully into the actual science behind various PPE strategies. The same Forbes writer who came out strongly against wearing masks in February walked that advocacy back on April 1st by saying "it's complicated"—and then proceeding to engage in a bit of self-contradiction:
Both the science and the pandemic itself have shifted and are continuing to shift. That article’s information was true at the time, and most of it remains true now.
There is no new scientific study that contradicts the findings of the studies already referenced here; the science has decidedly not changed. This is, of course, the only way her February 29 article's position could still be true.
It's Official: Masks Are Good
On April 3, the CDC revised its guidance to the general public to advocate wearing cloth masks.
It is critical to emphasize that maintaining 6-feet social distancing remains important to slowing the spread of the virus. CDC is additionally advising the use of simple cloth face coverings to slow the spread of the virus and help people who may have the virus and do not know it from transmitting it to others. Cloth face coverings fashioned from household items or made at home from common materials at low cost can be used as an additional, voluntary public health measure.
The cloth face coverings recommended are not surgical masks or N-95 respirators. Those are critical supplies that must continue to be reserved for healthcare workers and other medical first responders, as recommended by current CDC guidance.
While the CDC recommendation makes considerable reference to studies documenting asymptomatic and presymptomatic transmission for CCPVirus infections, it makes no reference whatsoever to any studies documenting any newfound efficacy of the community strategy of wearing masks. The extant scientific evidence provides no support for this strategy.
Even more remarkable is the CDC's explicit recommendation the general public wear cloth masks and not surgical masks or N95 respirators. On this point we have a 2011 study in Hanoi, Vietnam, which showed significantly higher infection rates for cloth masks over surgical masks or N95 respirators. The CDC's recommendation actually contradicts the science it is supposed to be using for all its decisions—the science it specifically promised to use while eschewing political considerations.
What is the basis for the CDC's revised recommendation? Merely that other nations were doing it.
With this announcement, the U.S. is following the lead of a number of other countries that have been urging — or outright ordering — their residents to don masks in public. The expanding list includes China and South Korea, where officials have even taken the step of distributing masks.
"Following the herd" is the epitome of a political decision, the very thing the CDC is precluded from making. That apparently is the sole foundation for the CDC's revised recommendation. It was and is a purely political statement, without regards to the underlying science.
The movement towards a community strategy of wearing masks is in actuality a consciously evidence-free policy. Several British healthcare experts have specifically acknowledged the lack of supportive evidence for the community strategy of wearing masks but also argued the lack of time to develop such evidence.
The BMJ has reported that the evidence is not sufficiently strong to support widespread use of facemasks as a protective measure against COVID-19. However, there is enough evidence to support the use of facemasks for "short periods of time by particularly vulnerable individuals when in transient higher risk situations".
Transient higher risk situations have been described by Prof Greenhalgh and others as: buses, trains, underground, supermarkets, pharmacies and any other places where social distancing cannot be easily maintained. Prof Greenhalgh advocated for widespread mask wearing, drawing an analogy with the 'precautionary principle' and suggesting that we should sometimes act without definitive evidence, just in case. She argued that in the face of a pandemic, the search for perfect evidence on the matter may be the enemy of good policy.
While the "precautionary principle" may be a rational basis for policy, the one thing it cannot be is scientific. The precautionary principle is in fact a statement of how to formulate policy and make decisions in the absence of scientific evidence.
Even the esteemed medical journal The Lancet acknowledges the lack of scientific foundation for the mask-wearing strategy.
However, there is an essential distinction between absence of evidence and evidence of absence. Evidence that face masks can provide effective protection against respiratory infections in the community is scarce, as acknowledged in recommendations from the UK and Germany. However, face masks are widely used by medical workers as part of droplet precautions when caring for patients with respiratory infections. It would be reasonable to suggest vulnerable individuals avoid crowded areas and use surgical face masks rationally when exposed to high-risk areas. As evidence suggests COVID-19 could be transmitted before symptom onset, community transmission might be reduced if everyone, including people who have been infected but are asymptomatic and contagious, wear face masks.
There is no scientific basis for this new-found support for the mask strategy, and yet nothing more than these statements by the "experts" has been sufficient to alter official public health guidelines and even to encourage elected officials to mandate wearing masks by the general public.
On April 15, Pennsylvania Governor Tom Wolf ordered masks be worn in all business establishments by both employees and customers alike. Businesses failing to comply would be effectively closed.
Businesses who fail to comply with the order risk the loss of their business license, fines, and citations. According to Wolf, state agencies including the Health, Agriculture, and Labor and Industry departments, the state police, Liquor Control Board, and local officials will enforce the order.
Governor Wolf's order, intruding as it does on the right of people to peaceably assemble on what is unquestionably private property (a business establishment) cannot possibly pass Constitutional muster, and certainly is bereft of any supporting scientific logic. Yet this is the burden Governor Wolf means to place on his citizens.
On April 22, Harris County Judge Lina Hidalgo issued an executive order mandating all people within Harris County, Texas, wear cloth masks when outside of their homes. Without even scientific foundation, nor legal foundation (which is why first the Houston Police Officers Union and then Harris County Sheriff's Deputies have taken a stand against enforcing the order).
Reality: Mask Mandates Are Not Effective
Despite the politics and the propaganda, there remains no hard data supporting the mask mandate. Quite the opposite.
A survey of Americans performed on July 23-26 by Morning Consult indicated at least 90% of Americans were wearing face masks out in public. This represented a significant increase in compliance from April.
Of those, 79 percent indicated that they “always” wear a mask, and 16 percent said they “sometimes” wear a mask. Mask-wearing has increased significantly in the last three months; in April, only 50 percent of adults indicated they were “always” or “sometimes” wearing a mask.
Nor was the compliance confined to any particular political or ideological demographic.
The current number of those who have indicated they are wearing masks remains relatively consistent across party lines: 98 percent of Democrats, 95 percent of independents, and 93 percent of Republicans.
However, the increased compliance has not coincided with a general decline in viral outbreaks in the United States, as on August 2 Dr. Deborah Birx, Coronavirus Response Coordinator for the White House Coronavirus Task Force, announced on CNN the virus was not contained in the US, blaming Americans' mobility as the culprit.
Dr. Deborah Birx said Sunday that the COVID-19 outbreak is not under control in the U.S. because Americans "are on the move."
If mask mandates were an effective mitigation, and 90% of Americans are complying with their community's mask mandates, how is it that CCPVirus remains "not under control" in the United States?
Mask mandates have been a demonstrable failure in the United States.
The Netherlands has gone so far as to refuse to enact a mask mandate, citing the lack of defensible scientific research to support the policy.
The decision was announced by the Netherlands Minister for Medical Care Tamara van Ark following a review by the country's National Institute for Health. Following a resurgence in cases over the past week or so, the Dutch government has decided it will instead seek better adherence to social distancing rules.
"Because from a medical perspective there is no proven effectiveness of masks, the Cabinet has decided that there will be no national obligation for wearing non-medical masks" Van Ark said.
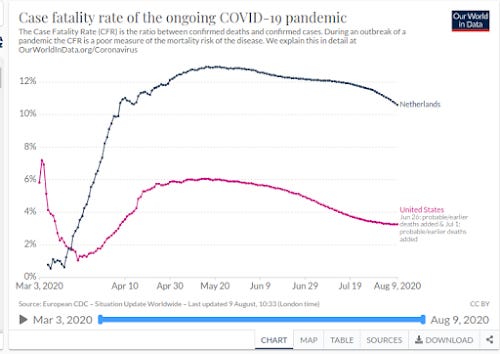
While the Netherlands does have a higher Case Fatality Rate than the United States, the trend and trajectory of their CCPVirus fatalities largely follows that of the US, indicating that masks indeed play no role in virus mitigation.
Moreover, Tamara Van Ark's assessment of a mask mandate is echoed by several of her peers across Europe, where there is a broad (and, it seems, growing) rejection of mask mandates as a disease containment strategy.
"All these countries recommending face masks haven’t made their decisions based on new studies," said Henning Bundgaard, chief physician at Denmark’s Rigshospitale, according to Bloomberg News.
Nor is Dr. Bundgaard's assessment unique:
Others, echoing statements similar to the US Surgeon General from early March, said masks could make individuals sicker and exacerbate the spread of the virus.
"Face masks in public places are not necessary, based on all the current evidence," said Coen Berends, spokesman for the National Institute for Public Health and the Environment. "There is no benefit and there may even be negative impact."
In Sweden, where COVID-19 deaths have slowed to a crawl, public health officials say they see "no point" in requiring individuals to wear masks.
"With numbers diminishing very quickly in Sweden, we see no point in wearing a face mask in Sweden, not even on public transport," said Anders Tegnell, Sweden’s top infectious disease expert.
The mask mandate is simply not a policy grounded in scientific research or empirical data. It is, as it has always been, a political, ideologically driven decision, supported not by science but by propaganda.
Fact: Not All Masks Are Created Equal
While we must acknowledge the mechanistic efficacy of some masks and mask materials—e.g., surgical masks and N95 respirators do block respiratory droplets, and they do deliver certain benefits within the hospital setting—we must also acknowledge that some mask materials are not effective at blocking respiratory droplets and do not deliver even the marginal benefit claimed by advocates of mask mandates. Some mask materials may even amplify droplet spread via aerosolization.
This is the conclusion of a survey of mask materials conducted by researchers at Duke University. Using laser measuring techniques, they assessed the capacity of various mask materials to block respiratory droplets. One interesting results of their survey was that certain types of fleece fabrics actually increased the number of droplets dispersed by breaking larger droplets into smaller droplets—a crude form of the process of aerosolization.
We noticed that speaking through some masks (particularly the neck fleece) seemed to disperse the largest droplets into a multitude of smaller droplets (see Supplementary Fig. S5), which explains the apparent increase in droplet count relative to no mask in that case. Considering that smaller particles are airborne longer than large droplets (larger droplets sink faster), the use of such a mask might be counterproductive.
Additionally, the authors of that study noted that, while valved N95 respirators reliably prevent the inhalation of various particulates, they do not actually inhibit the exhalation of respiratory droplets, which undermines their overall effectiveness in disease mitigation.
Furthermore, the performance of the valved N95 mask is likely affected by the exhalation valve, which opens for strong outwards airflow. While the valve does not compromise the protection of the wearer, it can decrease protection of persons surrounding the wearer. In comparison, the performance of the fitted, non-valved N95 mask was far superior.
A separate meta-study conducted at the University of New South Wales found that single layers of cloth were not effective at stopping the spread of the CCPVirus.
One study showed that a 12-layered cotton mask was as effective as a surgical mask, but a single-layered cloth mask was not protective against beta-coronaviruses.
Another meta-analysis of mitigation techniques published in The Lancet failed to established clear benefits for cloth masks:
Face mask use could result in a large reduction in risk of infection (n=2647; aOR 0·15, 95% CI 0·07 to 0·34, RD -14·3%, -15·9 to -10·7; low certainty), with stronger associations with N95 or similar respirators compared with disposable surgical masks or similar (eg, reusable 12-16-layer cotton masks; pinteraction=0·090; posterior probability >95%, low certainty).
That study did establish the utility of "social distancing" measures, with or without masks:
Transmission of viruses was lower with physical distancing of 1 m or more, compared with a distance of less than 1 m (n=10 736, pooled adjusted odds ratio [aOR] 0·18, 95% CI 0·09 to 0·38; risk difference [RD] -10·2%, 95% CI -11·5 to -7·5; moderate certainty); protection was increased as distance was lengthened (change in relative risk [RR] 2·02 per m; pinteraction=0·041; moderate certainty).
Staying away from sick people is unambiguously the best means to avoid getting sick, while the protection from wearing a mask is at best uncertain.
This is a far cry from the blanket insistence that masks work promoted by the CDC and other healthcare agencies.
The Word Of "Experts" Is Not Good Enough
Policy changes on the basis of the precautionary principle are not necessarily bad policy. Policy changes merely on the word of presumed "experts" is intrinsically bad policy.
Nowhere does the CDC acknowledge the policy change is driven by precaution rather than by hard science. In fact, the CDC, by making reference to studies documenting asymptomatic/presymptomatic transmission of CCPVirus and then recommending cloth masks be worn by the general public, is giving the clear implication that the mask strategy is supported by science—and it is not.
Nowhere does the CDC acknowledge the scientific evidence that illustrates the inefficacy of cloth masks. In effect, the CDC is making not just an unscientific recommendation, but an anti-scientific recommendation, and is doing so for purely political purposes.
Governors, elected officials, and the legacy media are in turn taking the CDC recommendation as holy writ and asserting that masks are now essential and making them mandatory.
Would it have been so improper for the CDC to formulate its recommendation specifically on the basis of the precautionary principle? Would it have been so wrong to say "we need to make mitigations now, and so we are issuing this guidance out of an abundance of caution while we research the strategy in light of the current pandemic"?
Had the CDC framed their recommendation along those lines, there would at least be a plausible foundation for community debate, for businesses and elected officials to weigh the merits and demerits of the mask strategy in their particular circumstances, and to effect workable public policy guidelines on the matter. Given the fascistic zeal of elected officials such as Tom Wolf in Pennsylvania and Lina Hidalgo of Harris County, Texas, there is little assurance they would have had sufficient self-reflection to engage in such public debate, but the role of the CDC is to facilitate and foster that debate, not to make politically popular recommendations that encourage excessive and lawless power grabs by government.
The CDC's mission is to use science to further the public health. With regards to the CCPVirus, it has substituted politics for science. This is going to harm the public health.
Experts are free to argue the policy and advocate the strategy on the basis of the precautionary principle. They are not free to call such advocacy "scientific" because it is not. No one should conflate an expert's policy stance with a statement of scientific principle, because it is not.
The word of experts may be many things, but it will never be science.
9 August 2020: Updated article with section reflecting current state of mask compliance in the US and perceived efficacy, along with the assessments of European health officials regarding mask mandates.
15 August 2020: Updated article with section documenting the variable mechanistic efficacies of different mask types and mask materials.