


I will confess, I am rather enjoying writing about monkeypox. It’s a nice change of pace from the serial soap operas into which US politics degenerated long ago. Plus it’s fun to play with epidemiological data!
Yes, I really am that much of a nerd.
Yet writing about monkeypox means I once again end up taking media to task for plain bad reporting. With disease outbreaks especially accurate information and clear communication is essential. Unsurprisingly, we aren’t getting that from the corporate media.
The BBC gets first dishonorable mention here, for this lamentable headline regarding “the first” recent monkeypox case in Sweden.

One would be forgiven for reading that headline and thinking that monkeypox was spreading in Sweden.
Of course, if one reads the article, the second sentence makes it clear that is not the case:
Sweden's public health agency has recorded what it says is the first case of a more dangerous type of mpox outside the African continent.
The person became infected during a stay in an area of Africa where there is currently a major outbreak of mpox Clade 1, the agency said.
The news comes just hours after the World Health Organization (WHO) declared that the outbreak of mpox in parts of Africa was now a public health emergency of international concern.
What happened in Sweden was that a person returned from a trip to Africa recently with a monkeypox infection in its incubation period.
This is unsurpising. In 2022 the incubation period for monkeypox was assessed at an average of between 8.51 and 9.1 days2. It takes on average a week and a half after infection for symptoms to appear.
Thus we have one person who traveled outside of Central Africa before showing symptoms. We do not have a fresh monkeypox outbreak erupting in Sweden.
Even worse, however, is that the BBC makes it seem as if monkeypox is not endemic in Sweden. Alas for poor Sweden, however, it is. We know that from the World Health Organization’s collected data on monkeybox.
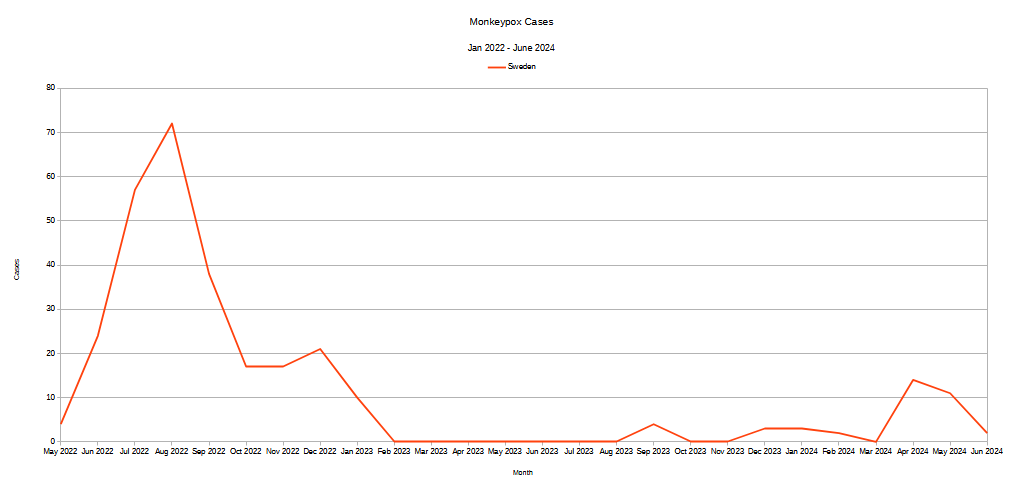
As happened with countries around the world in 2022, the global STD outbreak of monkeypox came to Sweden, and has stayed in Sweden, with an ongoing background level of cases continuing to occur—proving that the disease has taken up residence in Sweden and is now endemic.
This is an important detail, because the 2022 global STD outbreak of monkeypox involved the much less lethal Clade 2 strains, while the current outbreak in central Africa involves the more lethal Clade 1 and Clade 1b strains.
There are two types of Clade 1 and the Swedish case has been identified as Clade 1b. Since mpox Clade 1b was first witnessed in Democratic Republic of Congo there have been confirmed cases in Burundi, Kenya and Rwanda, before the new case identified in Sweden.
While Clade 2 did cause a public health emergency in 2022, it was relatively mild and some 300 cases have already been identified in Sweden.
While the single Clade 1b case in Sweden does not mean Clade 1b is now endemic there, it does mean that Sweden needs to pay attention to which Clade is the cause of a particular case of monkeypox. Obviously, Clade 1b becoming endemic in Sweden would be a significant change in the public health landscape.
More broadly, however, we should note with favor that the global corporate media is not, at least at present, spinning monkeypox into a new Pandemic Panic Hysteria. A Google News survey of world news stories as of this writing does not show any involving monkeypox. The same holds true for US stories: no monkeypox. Only when one zeroes in on Health stories does monkeypox command Google’s attention.
Corporate media is noting that European health officials are raising their threat assessment of monkeypox following, although Reuters is at present using measured and accurate language:
The European Centre for Disease Prevention and Control on Friday raised its risk level for mpox, a day after global health officials confirmed the first infection with a new strain of the virus outside Africa, in Sweden.
The EU public health body's head said there will be more imported cases of the new mpox strain in Europe in the coming weeks, though the risk of sustained transmission remains low.
All of which makes Jordan Schachtel’s headline for his Substack “The Dossier” needlessly inflammatory.

The WHO is a lamentable organization which is grotesque in its politicization of disease and public health. They are even more lamentable given, as I noted the other day, their studied indifference to monkeypox in Central Africa, where it has been an ongoing issue since before the 2022 global STD outbreak.

While a Clade 1 or Clade 1b outbreak of monkeypox within the United States will undoubted trigger a cascade of corporate media pearl-clutching and would have an impact on the dynamics of the current election cycle, at present that has not happened.
Where corporate media is heading with the monkeypox story is they are once again promoting vaccines as the savior of all mankind. Forbes was quick to highlight how Bavarian Nordic, the maker of JYNNEOS™, the current FDA approved monkeypox vaccine, is seeing its stock move higher on the news—because obviously they have an opportunity to sell more shots.
“The Conversation” dutifully trundled out a virologist, Cheryl Walter, to remind us that Africa was struggling with monkeypox because there were not enough doses of vaccine.
There are few resources to fight this disease and the shortage of vaccines is a major problem. The Africa Centres for Disease Control estimates there are only 200,000 doses available to African countries compared with a demand of at least 10 million.
However, there’s still a lot that can be done.
What both Ms. Walter and the Forbes article fail to address is that JYNNEOS is problematic as a monkeypox vaccine. As an orthopox vaccine it is only slightly better than its predecessor ACAM20003. It also does not appear to be very long-lasting, as booster shots are recommended every two years where people are at risk for repeated exposure (such as in Africa).
JYNNEOS’ efficacy at preventing infection is significantly lower than one might expect. During the 2022 global STD outbreak its efficacy was assessed at around 66%4. With one out of every three JYNNEOS vaccinations likely to fail, and with re-vaccination needed every two years, Africa is almost certainly understating the number of doses needed for an effective vaccination campaign.
What Ms. Walter also overlooks is that the 2022 global STD outbreak was not contained in the US through vaccines, but through behavior adaptation5.
Unlike Infectious Respiratory Diseases such as COVID, monkeypox requires contact with either an infected person or personal items such as soiled bed linens.
Person-to-person transmission of mpox can occur through direct contact with infectious skin or other lesions such as in the mouth or on genitals; this includes contact which is
face-to-face (talking or breathing)
skin-to-skin (touching or vaginal/anal sex)
mouth-to-mouth (kissing)
mouth-to-skin contact (oral sex or kissing the skin)
respiratory droplets or short-range aerosols from prolonged close contact
The virus then enters the body through broken skin, mucosal surfaces (e g oral, pharyngeal, ocular, genital, anorectal), or via the respiratory tract. Mpox can spread to other members of the household and to sex partners. People with multiple sexual partners are at higher risk.
Animal to human transmission of mpox occurs from infected animals to humans from bites or scratches, or during activities such as hunting, skinning, trapping, cooking, playing with carcasses, or eating animals. The extent of viral circulation in animal populations is not entirely known and further studies are underway.
People can contract mpox from contaminated objects such as clothing or linens, through sharps injuries in health care, or in community setting such as tattoo parlours.
This means that sanitation, hygiene, and isolation of infected individuals is effective against monkeypox—which the 2022 global STD outbreak demonstrated. Isolating an infected individual for the duration of the infection—typically 2-4 weeks6—will arrest the spread of the virus, with or without vaccination.
The DRC and other nations in Africa do not need additional doses of vaccine nearly as much as they need better sanitation and hygiene resources and expanded/improved facilities for properly isolating infected individuals so as to arrest viral spread. PPE and similar supplies would be far more immediately impactful in the DRC than vials of vaccine.
Downplaying this messaging in favor of vaccination, either for Africa or the rest of the world, is simply irresponsible journalism.
Monkeypox is not the “Election Variant”, but rather the latest “Big Pharma Advertising Variant”.
Where corporate media is coming up far short of where it should be is, as I mentioned previously, failing to highlight that monkeypox is not a “new” outbreak in Africa. It’s not a “new” outbreak in the Democratic Republic of Congo, where the Clade 1/1b variants predominate. The WHO’s own data sets make this abundantly clear.

Monkeypox in the DRC has been a growing problem really since before the 2022 global STD outbreak. Corporate media really should be ashamed of itself as it failed to make that point clear during the 2022 global STD outbreak as well.

With only problematic vaccines available, and not nearly enough doses of those to make a difference, the mission of the Africa CDC and WHO should have been all along to focus on the behavior aspects of how the 2022 global STD outbreak was tamped down without vaccines. Without saying the degree to which they did or did not make efforts in that regard, the data makes plain that any such efforts have failed.
Perversely, corporate media has likely missed a golden opportunity to crank up a fresh pandemic panic outbreak for the United States. What has been largely overlooked and not turned into a sensational and hysteria-producing headline is the fact that the WHO data shows the US has had more monkeypox cases than the DRC until just recently.
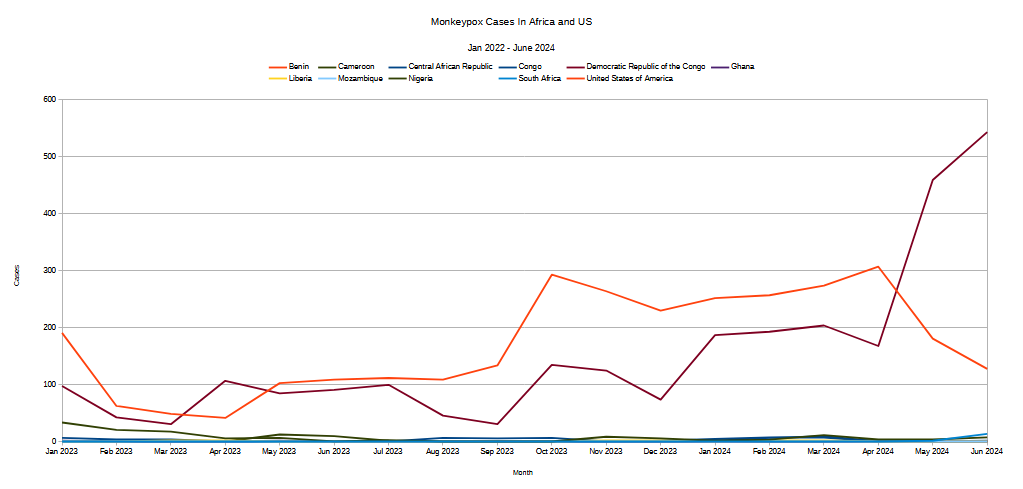
A couple of key points here: These are absolute numbers of cases, which means they do not take into account the United States’ greater population (346 million in the US vs 109 million in the DRC). They also do not reflect that the US cases are all Clade 2—echoes from the 2022 global STD outbreak—while the DRC cases are predominantly Clades 1 and 1b.
We should be glad the media is not seizing on this to generate a monkeypox hysteria here in the United States, although USA Today and some other news outlets have noted the fact.
There were no reported cases of clade I mpox in the U.S. as of Thursday. Federal officials say the risk is low, and Daigle said the CDC is monitoring the European case. A few cases of the less severe strain of the virus are still reported each week in the U.S.
At present, corporate media seems content to follow the Federal position that monkeypox Clade 1b is a low risk to the United States proper.
Not that some public health officials are not trying to generate hysteria. Ashwin Vasan, New York City Health Commissioner, is calling for the United States to “act quickly” in the wake of the WHO and Africa CDC public health emergency declarations.
On Thursday, Ashwin Vasan, New York City Health Commissioner, urged the country to act quickly to halt the spread of clade I, noting that “uncertainties cannot delay preparation, and the moment to act is now.”
“As we learn time and again, we are connected, and we cannot stand by and hope that another country’s suffering will not reach us,” Vasan said in a statement. “Prevention means we must be as invested in each other as we are in ourselves. It is not only moral and ethical, but also strategic.”
Vasan naturally ended his pearl-clutching and virtue-signalling with a call for more vaccines for everyone (surprise!)—monkeypox is the latest “Big Pharma Advertising Variant” after all.
Lamentably, Vasan’s statement itself was the epitome of the non-serious non-scientific pontification that passes for responsible commentary by public health officials today. Particularly obnoxious is his choice of framing how the 2022 global STD outbreak was contained as “pathbreaking”.
For the second time in just over two years, the World Health Organization has declared mpox a global health emergency. This action was necessary, and as the Health Commissioner of New York City – which was the epicenter of the mpox outbreak in the United States – we have learned many lessons from the 2022 outbreak, and we are prepared. While the current risk to New Yorkers and Americans is low, we must not only plan ahead but act now. In 2022, New York City introduced a range of pathbreaking interventions that were adopted all over the country. But it was not easy. Outbreaks are difficult to control, and it is sometimes challenging to predict exactly who will be affected. These uncertainties cannot delay preparation, and the moment to act is now.
Of course, what those “pathbreaking interventions” actually entailed was—yep, you guessed it!—more ways to vaccinate people.
In partnership with community, New York City consistently rolled out first-in-the-nation interventions. For example, New York City introduced a vaccination strategy that was followed nationally. In June 2022, using limited vaccine doses allocated to the City from the federal government, New York became the first jurisdiction to launch “extended PEP” vaccination clinics around Pride week – which opened vaccination to New Yorkers at risk of having had a recent exposure, rather than limiting to people who were a known contact of someone diagnosed with mpox. This innovative vaccine strategy opened a path for expanded vaccination access across the city and country. In addition, in response to concerns from partners, New York City was the first jurisdiction to call for an official change to the name monkeypox – and then eventually moving to unilaterally adopt a name-change for the city even before the WHO’s decision to update the name to mpox.
In the aftermath of COVID, reflexively trying to vaccinate everyone and their pet against monkepox is hardly an innovation.
That the vaccination campaigns were late and ineffective makes the continued crowing about them all the more absurd. Vaccines did not contain the global STD outbreak. People taking a few more cold showers and curtailing their random sex hookups did.
This has been something of a pet peeve of mine since the early days of the COVID Pandemic Panic Narrative. The early indicator that something was wrong with that narrative was that the data was not matching the media claims.

This should have been a major warning flag for private individuals as well as public health officials alike, because following the data and responding to that data should have been considered crisis management 101.

Unsurprisingly, we saw the same mistakes repeated during the 2022 global STD outbreak of monkeypox.

Public health officials are supposed to be effective at crisis communications—that’s an essential part of the job.
Corporate media types are supposed to be effective at communications, period. That is what journalism is meant to be all about: effectively communicating ideas and information to the wider audience.
Yet once again, crucial data is being ignored, data that significantly impacts how any media narrative might evolve:
This is not a “new” outbreak, nor even one that began earlier this year, but is one that has been ongoing for over two years.
This is not an outbreak which is global in scope. This is not a “global” crisis but an African one—and hopefully will remain that way.
JYNNEOS is not an highly effective vaccine and is not available in quantities needed for a mass vaccination campaign.
Non-pharmaceutical approaches to containing monkeypox were what brought the global STD outbreak to a halt in 2022. Vaccines came too late in the game to play a significant role. Minimizing exposure to infected bodily fluids is a mitigation which is immediately available to everyone without expensive vaccines or cumbersome logistics for medical supplies.
Monkeypox is not a new plague, and the world is not on the verge of a new pandemic. The world is not even seeing the need for an increased supply of JYNNEOS vaccine doses.
What the world is seeing is the extent to which indifferent and ineffective NGOs have failed to contain monkeypox (along with a number of other diseases) in Africa, and in the Democratic Republic of the Congo in particular. What the world is seeing is just how wasteful monies spent on these inept agences is.
What the world is seeing is the degree to which Africa (and the rest of the Third World) are routinely ignored and ill-treated by the very agencies created presumably to those countries.
Monkeypox is on the rise in the DRC now because the WHO and Africa CDC have failed to address it for at least the past two years. People are being sickened and a few are even dying because of the incompetence of the WHO and Africa CDC.
That’s what the data really shows, and that’s where the narrative should be focused.
Miura, Fuminari et al. “Estimated incubation period for monkeypox cases confirmed in the Netherlands, May 2022.” Euro surveillance : bulletin Europeen sur les maladies transmissibles = European communicable disease bulletin vol. 27,24 (2022): 2200448. doi:10.2807/1560-7917.ES.2022.27.24.2200448
Guzzetta, Giorgio et al. “Early Estimates of Monkeypox Incubation Period, Generation Time, and Reproduction Number, Italy, May-June 2022.” Emerging infectious diseases vol. 28,10 (2022): 2078-2081. doi:10.3201/eid2810.221126
Rao AK, Petersen BW, Whitehill F, et al. Use of JYNNEOS (Smallpox and Monkeypox Vaccine, Live, Nonreplicating) for Preexposure Vaccination of Persons at Risk for Occupational Exposure to Orthopoxviruses: Recommendations of the Advisory Committee on Immunization Practices — United States, 2022. MMWR Morb Mortal Wkly Rep. ePub: 27 May 2022. DOI: http://dx.doi.org/10.15585/mmwr.mm7122e1
Deputy, PhD, N. P., et al. “Vaccine Effectiveness of JYNNEOS against Mpox Disease in the United States.” The New England Journal Of Medicine, vol. 388, no. 26, 2023, doi: 10.1056/NEJMoa2215201.
Bunge, Eveline M et al. “The changing epidemiology of human monkeypox-A potential threat? A systematic review.” PLoS neglected tropical diseases vol. 16,2 e0010141. 11 Feb. 2022, doi:10.1371/journal.pntd.0010141
Huang, Yong et al. “Monkeypox: epidemiology, pathogenesis, treatment and prevention.” Signal transduction and targeted therapy vol. 7,1 373. 2 Nov. 2022, doi:10.1038/s41392-022-01215-4
You keep right on being a data nerd, Peter - that hard data is TRUTH! (Or at least good indications of truth.) Your passion for illuminating the pertinent facts is GOLDEN.
A pet peeve of mine is that the media is filled with people who majored in Journalism or Communications or English. Most of them have zero education in the actual subjects they are writing about. They can’t tell if they are being manipulated by a corporation’s public relations department because they don’t understand what they are being told. Frequently they end up looking like incompetent fools because of their ignorance.
My undergrad degree was in geological engineering, so I’ve been educated in the basics of plate tectonics and earthquakes. It seems like every time I’ve read an article in the MSM about an earthquake, the writer had no idea of what he or she was saying. There was no understanding of the logarithmic scale of the Richter scale, no comprehension of the 3D nature of fault-line interaction, no grasp of the fact that the depth of a quake makes all the difference in the amount of damage done. I mean, it’s common sense that a quake centered 2 miles down is going to do more damage than one that’s centered 40 miles down, right? Yet the ‘journalist’ doesn’t even grasp that! “Earthquake in LA”!, screams the headline. Pffsst. It’s 3.9 on the Richter scale and 30 miles down. A large truck driving past your house will rattle your teacups more than that quake, and that journalist just made himself look like a fool to every geologist in the world.
In other words, we need more intelligent, educated writers who can THINK - people like you, Peter. Thanks!
this is a thorough examination of the media coverage surrounding monkeypox. The issues you've highlighted, from media misrepresentation to potential conflicts of interest, raise important questions about the accuracy and transparency of the information being provided to the public.
It's troubling to think that public health messaging could be influenced by pharmaceutical interests, especially when effective, non-pharmaceutical interventions may be overlooked. It's vital that we strive for accurate, balanced reporting to inform the public about health threats without causing undue panic or contributing to misinformation.