

New York Post Smears RFK,Jr. On COVID Claim
Reports What RFK Didn't Say, Not What He Did Say

The first thing to understand about the New York Post story claiming Robert F. Kennedy, Jr, said COVID was an “ethnically targeted” bioweapon is that is it is journalistic garbage. About the only thing factual in the story is the video clip of Kennedy making comments in an informal setting about COVID.
Democratic presidential candidate Robert F. Kennedy Jr. dished out wild COVID-19 conspiracy theories this week during a press event at an Upper East Side restaurant, claiming the bug was a genetically engineered bioweapon that may have been “ethnically targeted” to spare Ashkenazi Jews and Chinese people.
How well Kennedy stated the scientific research on this point is debatable, but saying that there is an argument to the effect the SARS-CoV-2 virus is a genetically engineered bioweapon is neither semantically nor logically the same as staking that argument as an actual claim. New York Post reporter Jon Levine surely knows the difference, and simply disregarded it in favor of a propagandistic “spin” on Kennedy’s comments that is not at all accurate.
Levine spun an entire story about what RFK, Jr., didn’t say, while completely overlooking the story about what he did say.
That SARS-CoV-2 is a bioweapon is hardly a new debate topic. The bioweapon hypothesis of the virus’ orgins emerged practically at the same time the virus emerged, and was a topic of significant discussion and research within the alternative media in early 2020.

Today's "conspiracy theory" can all too quickly become tomorrow's substantive fact.
We must bear this in mind when considering the most disturbing "conspiracy theory" we have yet on COVID-19: that the virus is a laboratory construct, a bioweapon released either by accident or by design.
That the SARS-CoV-2 virus may very well have emerged from a Chinese biolab is no longer a “conspiracy theory”, but a widely shared consensus viewpoint, as Senator Marco Rubio went to great lengths to document earlier this spring.

To describe a discussion about the virus as a bioweapon as “wild COVID-19 conspiracy theories” is to disregard this very real and relevant context. Such dismissal of the current state of public discourse about the virus is inexcusable from any journalist, corporate, alternative, or independent.
Fortunately, the New York Post included a video clip of Kennedy making his comments, and so we have the advantage of knowing verbatim what he said. We need not rely on Jon Levine’s errant interpretation. For convenience, a transcription of the video, generated using the Go Transcribe online transcription service, is included below1.
What Kennedy did say is that “COVID-19 is targeted to attack Caucasians and black people.” He further elaborated that “the people most immune are Ashkenazi Jews and Chinese”.
What Jon Levine said about these statements is factually false:
Kennedy’s remark echoes well-worn anti-Semitic literature blaming Jews for the emergence and spread of coronavirus which began circulating online shortly after the pandemic broke out, according to The Center for the Study of Contemporary European Jewry at the University of Tel Aviv’s 2021 Antisemitism Worldwide Report.
Given that Kennedy preceded his statements about how COVID-19 targeted specific groups with the observation that “The Chinese have done the same thing [develop ethnically targeted microbes]”, one cannot conclude that Kennedy is implying that “Jews” are somehow inherently responsible for the emergence of SARS-CoV-2. Levine also is guilty of some terminological slovenliness in referring to “coronavirus” in relation to these anti-Semitic tropes. “Coronavirus” is a family of viruses, of which several—including SARS-CoV-2—are known to cause Influenza-Like Illness in human beings. This is an immediate clue that Levine is playing fast and loose with the facts.
Moreover, Levine’s reflexive corporate media denigration of “no evidence” is also factually false even within the video clip itself.
There has been a growing consensus among US intelligence agencies that COVID-19 was man-made and escaped from a lab in Wuhan, China — but there is no evidence it was designed to spare certain religious groups or ethnicities, and Kennedy offered no studies to support his claims.
Quite the contrary, Kennedy began the clip by pointing out he had been researching a book on bioweapons for two and a half years, and specifically said that “there are papers out there” regarding the assertions Kennedy was making—which is a reasonable statement for Kennedy to make if he’s been doing book research on the topic for the past two years. He would know about the papers because he’s likely come across them and even read them.
We must pause to remember that, by Levine’s own reporting, this was an extemporaneous conversation over dinner. Even an obnoxious data geek such as myself does not in dinnertable conversation include an MLA-compliant footnote referencing a specific research study; generally it is considered adequate to make reference to the existence of studies, and if people are curious, then one can develop the details of that further.
As it turned out, Kennedy had those details, as he included a link to the study in question in a tweet he put out slamming Levine for misreporting the conversation.

Kennedy reiterated this point in an article on his Substack further rebutting Levine’s misreporting of his statements.

I have never, ever suggested that the COVID-19 virus was targeted to “spare” Jews. I accurately pointed out — during an off-the-record conversation — that China and other governments are developing ethnically targeted bioweapons and that a 2021 study of the COVID-19 virus shows that COVID-19 appears to disproportionately affect certain races since the furin cleave docking site is most compatible with Blacks and Caucasians and least compatible with ethnic Chinese, Finns, and Ashkenazi Jews.
In that sense, it serves as a kind of proof of concept for ethnically targeted bioweapons. I do not believe and never implied that the ethnic effect was deliberately engineered.
Sadly, by not bothering to search out that study and read it himself, Levine managed to completely miss a real and relevant story regarding possible dimensions and implications of the growing body of evidence that SARS-CoV-2 is a laboratory-engineered virus, that it may even have been manipulated at a molecular level, and that it potentially is a biological weapon in the purest sense of the term:
a harmful biological agent (such as a pathogenic microorganism or a neurotoxin) used as a weapon to cause death or disease usually on a large scale
If the virus was deliberately released then it is by definition a bioweapon, and with the evidence of lab construct steadily mounting, this is a possibility we can no longer discount. It was an important story in 2020, and it is an even more important story now in 2023.
Which brings us to the study in question, and Kennedy’s understanding of it.
Kennedy was referring to a study2 (the Hou study, after the lead researcher) which appeared in BMC Medicine in July, 2020.
The date of publication is important to note, as this was research done early on in the pandemic. As was apparent even in the earliest days of the pandemic, the ramifications implied by much of that early research frequently did not pan out as the pandemic progressed. We saw this almost immediately in 2020, when the projected severity ratios of cases did not pan out anywhere outside of China.

Caution must be taken, therefore to compare what a study appears to indicate about SARS-CoV-2 infection against what has been recorded in overall test and case data worldwide—which thankfully we do have. As happened more than once, the breakdowns of disease distribution and predictions of immunity vs susceptibility implied by the Hou study does not align with real world data.
What the Hou study examined in particular was the role human genetic factors played in susceptibility to the SARS-CoV-2 virus, and it is their appraisal of the relevant factors and their ethnic distributions which Kennedy attributes as proof of differential ethnic impact.
Coronavirus Disease 2019 (COVID-19), caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), has now been confirmed worldwide. Yet, COVID-19 is strangely and tragically selective. Morbidity and mortality due to COVID19 rise dramatically with age and co-existing health conditions, including cancer and cardiovascular diseases. Human genetic factors may contribute to the extremely high transmissibility of SARS-CoV-2 and to the relentlessly progressive disease observed in a small but significant proportion of infected individuals, but these factors are largely unknown.
This study took a closer look at the role angiotensin-converting enzyme 2 (ACE2) and the host transmembrane serine protease TMPRSS2 plays in susceptibility to SARS-CoV-2 infection, building off an April, 2020, study3 which appeared in Cell which detailed the importance of ACE2 and TMPRSS2 in the spread of COVID. In particular, the study sought to establish a genetic basis for how to approach variations in ACE2 and TMPRSS2 in identifying effective therapeutics and treatment strategies against COVID.
Therefore, a systematic investigation of the functional polymorphisms in ACE2 and TMPRSS2 among different populations could pave the way for precision medicine and personalized treatment strategies for COVID-19.
One of the variance distribution dimensions they identified was by ethnic/genetic grouping.
We found that the distribution of deleterious variants in ACE2 differs among 9 populations in gnomAD (v3). Specifically, 39% (24/61) and 54% (33/61) of deleterious variants in ACE2 occur in African/African-American (AFR) and Non-Finnish European (EUR) populations, respectively (Fig. 1b). Prevalence of deleterious variants among Latino/Admixed American (AMR), East Asian (EAS), Finnish (FIN), and South Asian (SAS) populations is 2–10%, while Amish (AMI) and Ashkenazi Jewish (ASJ) populations do not appear to carry such variants in ACE2 coding regions (Fig. 1b).
This is to what Kennedy was referring when he spoke of Chinese and Ashkenazi Jews being immune.
However, this study was grounded on the viral strains present in early 2020 and on what was understood about them in 2020. It matters, therefore, that the genetic variations for ACE2 and TMPRSS2, and the ethnic distributions observed for those variations, do not reconcile with observed patterns of both infection and mortality that emerged throughout 2020. In particular, while the Hou study indicates that Ashkenazi Jews do not have susceptibility (or have reduced susceptibility) to SARS-CoV-2, we see Israel, which has a significant Ashkenazi Jewish population, having significant waves of infection by the SARS-CoV-2 virus throughout 2020. We also see other countries having significant waves of infection contrary to the implied immunities the Hou study indicated should exist.
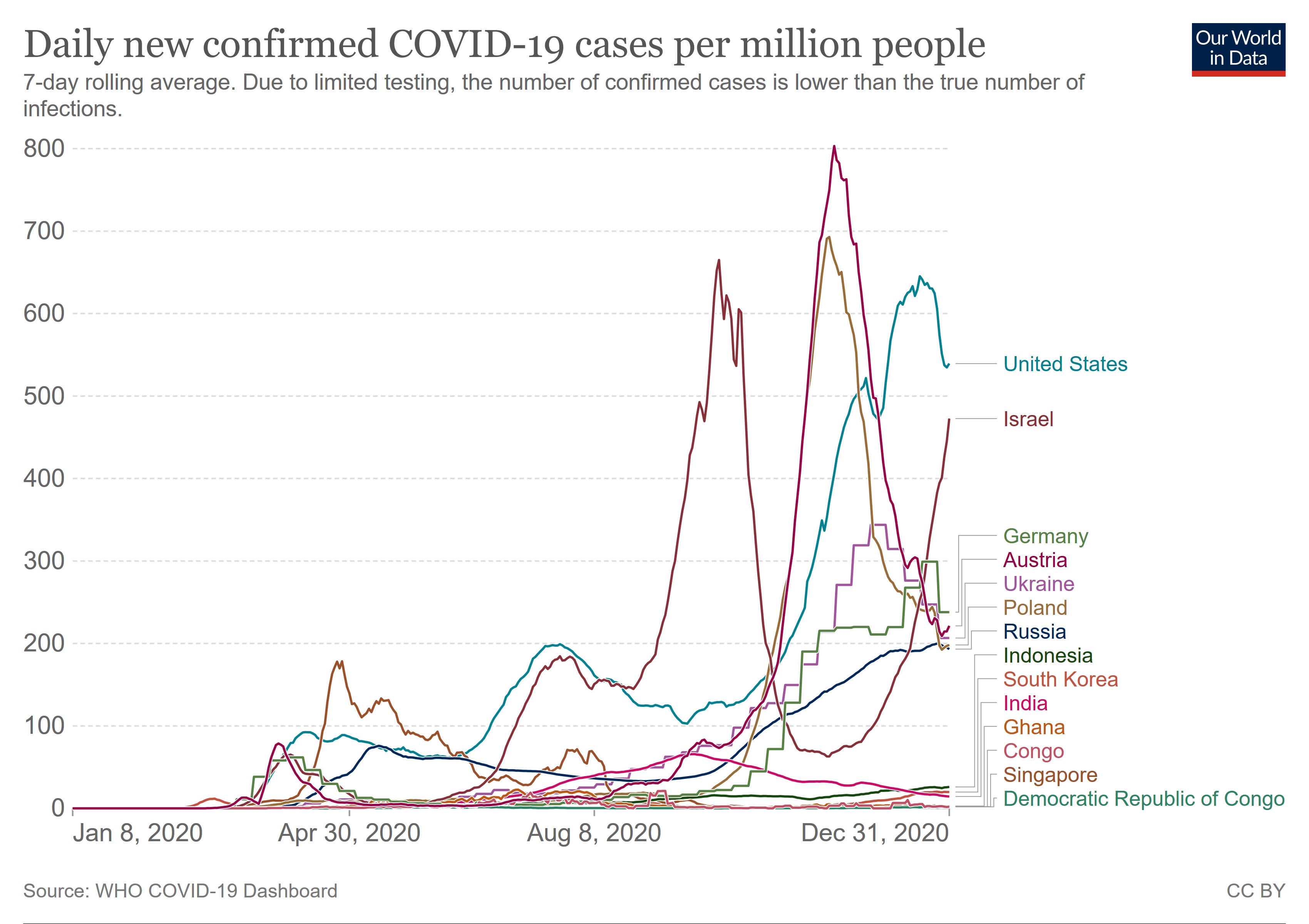
When we look at cumulative cases throughout 2020, the trends are unmistakable.

The significance of these charts lies in the countries listed. Israel has the second largest population of Ashkenazi Jews in the world (the US has the largest), Singapore is populated mainly by ethnic Chinese, while Ghana, Congo, and Democratic Republic of Congo are obviously African countries. While it is an oversimplification to suggest that these countries are perfect representatives of the ethnic populations described briefly in the Hou study, they are reasonable approximations of them, and yet one of the populations with the largest percentages of deleterious ACE2 variations—Africans/African Americans—had the lowest numbers of cases relative to population throughout 2020. Israel, with its large population of Ashkenazi Jews, had one of the highest numbers of cases relative to population.
If we apply Kennedy’s interpretation of the Hou study, these outcomes should not have happened.
If we look at COVID deaths in 2020, we see similarly counterintuitive results.

While Israel’s mortality from COVID was not the leading number that it was for cases, their mortality is still significant, and the African countries’ mortality is still relatively insignificant.
Cumulative numbers tell a similar tale.

It is not possible, as a matter of empirical observation at a country level, to say that Ashkenazi Jews have demonstrated significant immunity to COVID or are less vulnerable to severe infection and death from COVID. It certainly is not possible to say that African nations have greater risk of infection and death from COVID than Israel, and thus that Africans have greater such risk than Ashkenazi Jews. Certainly during 2020—the time frame when the original Wuhan strain of the virus was dominant rather than the subsequence variants of concern (i.e., Delta and Omicron)—the risk of COVID to various ethnic groups and genetic haplogroups is significantly different than what the Hou study appears to imply.
Even within the United States, the CDC weekly case data does not line up all that well with the results of the Hou study. In 2020 and early 20201, the ethnic group most impacted by COVID was the Hispanic population, with American Indian and indigenous populations also being significantly impacted.

This presentation of COVID contradicts the risks and vulnerabilities of these ethnic groups as assessed by the Hou study. According to how Robert Kennedy appears to apprehend this study, what the study predicted would happen with regards to the ethnic impact of the SARS-CoV-22 virus is not what actually did happen.
However
Before dismissing both the Hou study as flawed research and RFK for doing seemingly flawed research into the topic of bioweapons, we need to reflect on something else RFK said in that video.
We the technology that we now have to develop these microbes, we have we've put hundreds of millions of dollars into ethnically targeted microbes.
Kennedy restates the same point in his Substack rebuttal to Jon Levine.
In that sense, it serves as a kind of proof of concept for ethnically targeted bioweapons. I do not believe and never implied that the ethnic effect was deliberately engineered.
To understand the broader thesis Kennedy is developing here, consider what the Hou study shows is possible versus what the epidemiological data showed actually happened:
In the Hou study, Ashkenazi Jews and Chinese would have the lowest risk for SARS-CoV-2 infection, as those ethnicities do not have the susceptible ACE2 variants.
In the Hou study, Africans/African Americans and Europeans would have the greatest risk. Latino and Hispanics would have significantly less risk, although more than Chinese people.
In the empirical data, during 2020, the country of Israel, which has a sizeable population of Ashkenazi Jews, had a higher incidence of infection than many other countries, including many African nations—many of which had considerably lower incidence of infection relative to Israel or even Singapore. Singapore, being predominantly ethnic Chinese, arguably should not have ever had a significant outbreak of COVID.
In other words, the ethnic distribution of actual infection risk is in many ways almost opposite of the implied distribution of infection risk from the Hou study—but there is still ethnic distribution of actual infection risk.
What is the significance of this?
First, it is significant that there have been significant ethnic variations in infection risk and incidence of SARS-CoV-2 infection. No, the variations are not what at least the Hou study modeled, but there are ethnic variations, and that is the broader point Kennedy is making. While the empirical data contradicts the Hou study, is also to some degree confirms Kennedy’s notion that ethnically targeted viruses are possible.
Additionally, given the accumulation of evidence indicating the SARS-CoV-2 virus originated from the Wuhan Institute of Virology, a biolab with known connections to the Chinese military (which almost certainly means it conducts bioweapons research) as well as documented funding by the US NIH for gain-of-function research, the possibility that the characteristics of the virus which target ACE2 receptors in the body are deliberate and intentional cannot be ignored.
The Hou study indicates that a virus with a disparate impact on various ethnic populations is at least potentially possible. Robert Kennedy in that video clip asserted that both the US and China are working on ethnically targeted bioweapons. Given the deceptions, the fraud, the lies which we have seen just from the FDA, NIH, and CDC over SARS-CoV-2, is Kennedy’s assertion outlandish or impossible to imagine? Not in the slightest—it is all too probable.
The empirical epidemiological data shows that SARS-CoV-2 is not so much a “proof of concept” of this, but rather proof of how difficult it would be to have a particular ethnically associated characteristic of a manufactured bioweapon have the desired ethnic impact. Yet the empirical epidemiological data also tells us that ethnic impact is very much a potentiality of any manufactured “Frankenvirus”’; that which is difficult is also that which is ultimately possible. Even if SARS-CoV-2 should be eventually prove to be an wholly naturally occurring virus which arose naturally and learned to infect people, what Mother Nature has done, man is certainly capable of figuring out how to do. If SARS-CoV-2 is in fact man-made, the “pandemic” ultimately is but an illustration of how much more “figuring” man has yet to do on such a creation.
Bear in mind also that we know already that the United States has spent untold billions on a variety of “threat reduction” and “biosafety” initiatives, the research outcomes of which are too often “classified” and hidden away from the general public.

We have seen through events like the post-9/11 anthrax attacks that “threat reduction” is easily turned into “threat creation”.
We know that even now virologists in multiple countries are routinely playing God with viruses.

The extent to which this research is or is not “bioweapons” research is largely a matter of cynical semantics and Clintonian word parsing. All viral research, and in particular gain-of-function research, has the potential to devise new ways for people to do great harm to one another.
Even Pfizer has more or less admitted to performing gain-of-function research.

With such things already known and proven, the assertion that governments are researching ethnically targeted pathogens hardly stretches the bounds of credibility. With research such as the Hou study in hand, if there is not such research currently taking place it is only a matter of time before it does—which means that even if Robert Kennedy is wrong about such research today, the odds are heavily in his favor that he will be right about it tomorrow.
With such things already known and proven, Kennedy’s two minute foray into the state of bioweapons research is neither the stuff of a crank nor the stuff of a conspiracy theorist. The degree to which SARS-CoV-2 was intended in its creation to be a bioweapon and the degree to which the pandemic panic which followed its creation was what was weaponized is little more than a discussion over details.
Robert F. Kennedy, Jr., is right about at least this much: we do need to talk about bioweapons. We need to talk about how our government is spending our tax dollars enabling virologists to play God with viruses with little or no accountability.
Jon Levine could have chosen to pursue that story. He could have taken Robert Kennedy at face value when he said “we have to talk about bioweapons”. He could have followed Kennedy’s advice and helped initiate that larger talk about bioweapons. Instead he attempted to dismiss and denigrate Kennedy, seeking to marginalize him as a crank and a conspiracy theorist when the facts show that he is neither.
RFK’s video-recorded comments on COVID, as transcribed:
And we need to talk about bio weapons. I know a lot now about bio weapons because I've been doing a book on it for the past two and a half years. And and you know what? We the technology that we now have to develop these microbes, we have we've put hundreds of millions of dollars into ethnically targeted microbes. The Chinese have done the same thing. In fact, Covid 19, there's an argument that it is ethnically targeted. Covid 19 attacked certain races disproportionately. The the races that are most immune to Covid 19 are because of the structure of the of the genetic structure of different genetic differentials among different races of the of the receptors of the ace2 receptor. Covid 19 is targeted to attack Caucasians and and and black people. The people who are most immune are Ashkenazi Jews and and Chinese. And we don't know whether it was deliberately targeted that or not. But there are papers out there that show the, you know, the the racial and ethnic differential in impact to that. We do know that the Chinese are spending hundreds of millions of dollars developing ethnic bioweapons and we are developing ethnic bioweapons. That's what all of those labs in the Ukraine are about. They're collecting Russian DNA. They're collecting Chinese DNA that we can target people by race.
Hou, Yuan et al. “New insights into genetic susceptibility of COVID-19: an ACE2 and TMPRSS2 polymorphism analysis.” BMC medicine vol. 18,1 216. 15 Jul. 2020, doi:10.1186/s12916-020-01673-z
Hoffmann, Markus et al. “SARS-CoV-2 Cell Entry Depends on ACE2 and TMPRSS2 and Is Blocked by a Clinically Proven Protease Inhibitor.” Cell vol. 181,2 (2020): 271-280.e8. doi:10.1016/j.cell.2020.02.052
Thank you for the clarification. RFK has a knowledge and understanding of these issues which would be difficult to put into lay terms, however you did it quite well, possibly best of all.
-Edwin
RFK Jr is taking flak from all angles - must be onto something (many things).