For so many notionally educated and informed people to swan dive into the cesspool of collective ignorance that is the font of all propaganda is truly a depressing reality. Yet it is the reality we have.
This is what the monkeypox “emergency” has gifted us—a pandemic of virtue signalling and self-righteous posing and preening by the “woke” among us.
Declaring a virus that is almost completely non-lethal1, is spread almost entirely by intimate sexual contact, and to which one is susceptible only if one fails to practice basic self-discipline, basic self care, and basic self-restraint, a public health emergency has been nothing less than a siren call to those who wish freedom not from tyranny but from consequence—a freedom that does not exist nor ever has existed.
Monkeypox “Can” Infect Anyone…It Just Happens To Prefer The Promiscuous
One does not need to wonder about the agendas of the virtue-signallers when it comes to monkeypox or any other “health emergency”—they’re happy to spell it out for you.
But while infectious disease experts urge men who have sex with men in cities, like St Louis, not yet hit hard by monkeypox to educate themselves on the disease, they also warn against panic, an understandable reaction for a demographic that was torn apart by the Aids epidemic.
“I think it would be safe to say that this could be stressful for individuals, on top of two and a half years of incredible stress,” said Dr Preeti Malani, an infectious disease specialist at the University of Michigan. “People should be worried but not to the point where they are not able to move forward with their lives.”
The suspected means of monkeypox virus transmission as reported by the clinician was sexual close contact in 95% of the persons. It was not possible to confirm sexual transmission. A sexual history was recorded in 406 of 528 persons; among these 406 persons, the median number of sex partners in the previous 3 months was 5 partners, 147 (28%) reported travel abroad in the month before diagnosis, and 103 (20%) had attended large gatherings (>30 persons), such as Pride events. Overall, 169 (32%) were known to have visited sex-on-site venues within the previous month, and 106 (20%) reported engaging in “chemsex” (i.e., sex associated with drugs such as mephedrone and crystal methamphetamine) in the same period.
Are these the things that are meant when encouraging people to “move forward with their lives”?
Based on the data, the people most at risk of catching monkeypox are those who engage in promiscuous sexual behaviors. It really does have very little do to with sexual orientation, and quite a lot to do with sexual self-discipline and sexual self-control.
“Intimacy” Is Not “Sex”
Does this mean that people should refrain from sexual activity? Not really. It does mean that reckless sexual behavior is—and has always been—a preventable health risk. It is also a reminder that sexual intimacy is—and has always been—a matter to be approached with a measure of care and seriousness.
People are well advised to reflect on what the word “intimate” means—and what it is supposed to mean.
marked by a warm friendship developing through long association
The characteristic of a “warm friendship” shows that “intimacy” is intrinsically psychological and emotional, rather than physical. That emotional element differentiates that which intimate fom that which is purely recreational.
Given that monkeypox generally resolves itself within a month or so, with just a little care and basic hygiene precautions it should not be any sort of impediment to developing an intimate connection with someone—that process by definition takes time, and time is not the monkeypox virus’ friend.
However, not everyone pauses to reflect on that denotative2 meaning of “intimate”, focusing instead on its later connotative meaning linking it to all things sexual, even activity which is casual and purely recreational.
engaged in, involving, or marked by sex or sexual relations
“It will have a continual impact on my intimate side of life,” said Brinkman, who lives in a St Louis suburb and is retired after working in information technology. “I don’t have anybody in my life right now, and to try to meet somebody on that level, it raises a big concern, and I think a lot of people are thinking about that too.”
Nor is it a rare and infrequent appearance. From an op-ed in The Guardian:
I realized in that moment how lucky I am to have a gay doctor’s office to take my body and my feelings seriously. And I realized how angry I was that, for the third time in my life, a viral pandemic was dictating my sex life, shaping my professional life, messing with my head, and keeping me from experiencing intimacy.
Again, as “intimacy” emerges over time through long association, and as monkeypox typically lasts 2-4 weeks, it is not rational to argue that the virus can prevent anyone from "experiencing intimacy”. Going to “sex-on-site” venues is not seeking or experiencing “intimacy”, but merely looking for a “booty call”.
How much friendship and warmth can develop if one is moving from sex partner to sex partner at a rate of 5 every three months or so?
Moreover, some doctors and clinicians are, for whatever reason, giving out muddled messages regarding monkeypox, sexual activity, and intimacy. Consider this bit of introspection from Jay Varma, the director of the Cornell Center for Pandemic Prevention and Response (emphasis mine):
“Whenever we talk about sex, we as healthcare providers always need to recognize that sex has health benefits, and it brings joy to people’s lives,” said Varma. “That said, you also need to be realistic and honest about where risk is right now. And at the moment … the highest risk is from either anonymous sex partners and/or sex-related events where people are having sex with multiple partners, so it is wise for men who have sex with men to be thinking about what their risk tolerance is.”
Again, if “intimacy” is a warm friendship that develops over time, how can there be any intimacy when one’s sexual partners are anonymous? Or if one is having sex with multiple partners?
Denying Reality
When 99% of monkeypox cases outside of Africa are among gay and bisexual men, it is absurd to claim there is no linkage between that demographic and the virus. Yet many activists insist on exactly that claim.
Last week, WHO Director-General Dr Tedros Adhanom Ghebreyesus had said: “For men who have sex with men, this includes, for the moment, reducing your number of sexual partners, reconsidering sex with new partners, and exchanging contact details with any new partners to enable follow-up if needed.”
On Monday, the global health body clarified: “It is important to note that the risk of monkeypox is not limited to men who have sex with men. Anyone who has close contact with someone who is infectious is at risk.”
LGBTQ activist Yadavendra Singh told ThePrint that it was “very unfortunate that the WHO DG linked monkeypox to multiple gay sexual partners”.
In the United States, cases of monkeypox are widely distributed across the country, although most cases are concentrated in three large cities. While a few cases have occurred in children and a pregnant woman, 99% are related to male-to-male sexual contact.
In Canada, 99% of cases have occurred among MSM, and the country is taking a broad approach to pre-exposure prophylaxis, given the challenges with contact tracing; and is strongly focused on engagement with community-led organizations supporting key affected populations groups.
Nigeria recorded a little over 800 cases of monkeypox between September 2017 and 10 July 2022 and has seen at 3% case fatality ratio among confirmed cases. Cases are predominantly in men aged 31 to 40 years; there was no evidence of sexual transmission presented. The highest number of annually reported cases since 2017 has been observed in 2022.
99% of cases is as strong a link as one is ever likely to find. While it is quite possible for the virus to be passed among men and women, the reality thus far is that the virus is concentrated almost exclusively among gay and bisexual men. Even after multiple generations of the virus, and multiple transmissions of the virus from host to host, that link remains very much part of the present reality.
African Cases Show Where The Real Discrimination Is Occurring
Although the WHO and the corporate media rather sloppily lump the outbreak in Africa with the global outbreak, the clear differences between the African cases and the cases beyond Africa not only demonstrate that there are in reality two distinct outbreaks, but also the relevance of sexual activity in the global outbreak.
Ogwell said health officials in Africa have collected data on monkeypox since 1970 and that men who have sex with men has never come up as a significant issue. He said the drivers of this outbreak are “traditional” ones, including close contact in confined spaces and living in communities in contact with animals that have the virus.
“We have not seen any evidence of any specific group of persons being affected by monkeypox,” he said. “All communities, all ages, all genders are at risk.” He urged people to “avoid definitions and communications that may stigmatize those exposed.”
This lack of a sexual context for cases in Africa serves to highlight the degree to which sexual activity is playing a key role in the transmission of the virus beyond Africa. It highlights at least some of the ramifications of the extraordinary number of mutations that have been observed in monkeypox from cases beyond Africa.
Sadly, the African cases also demonstrate how biased and politicized the WHO is when it comes to responding to outbreaks of infectious disease. As I noted back in June, Africa has had an ongoing outbreak of monkepox since the beginning of the year—and arguably since 2017—one in which a number of deaths has been recorded, yet the WHO did not consider that to be a public health emergency.
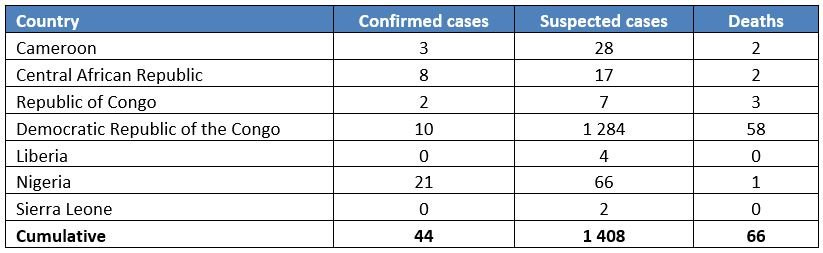
In addition to the cases reported from or identified in non-endemic countries, WHO continues to receive updates on the status of ongoing monkeypox outbreaks in endemic countries[1] in the African region through established surveillance mechanisms (Integrated Disease Surveillance and Response). From January to 1 June 2022, 1408 suspected and 44 confirmed cases including 66 deaths were reported from seven endemic countries (Table 2).
[1] Monkeypox endemic countries are: Cameroon, the Central African Republic, the Democratic Republic of the Congo, Gabon, Ghana (identified in animals only), Cote d’Ivoire, Liberia, Nigeria, the Republic of the Congo, and Sierra Leone. Benin and South Sudan have documented importations in the past. Countries currently reporting cases of the West African clade are Cameroon and Nigeria.
Table 2. Cases of monkeypox in the WHO African Region reported to WHO from 1 January 2022 to 1 June 2022
The WHO even now refuses to acknowledge the suspected cases within Africa, despite an increase of 766 confirmed and suspected cases just within the past week, with some 28 suspected deaths from the disease. The WHO Health Emergency Dashboard shows none of those cases.
For those concerned about discrimination and “stigmatization” of those afflicted with monkeypox, that’s where it’s actually happening—in Africa, where people have been dying from the disease since before it spread beyond Africa, and have been largely ignored by the same WHO that decided that monkeypox becoming a new STD was a global crisis.
Again, Monkeypox Is Not A “Public Health Emergency”
What I have said before I shall say again—and keep on saying for as long as its true and relevant: monkeypox is a concern, but it is not an emergency. It certainly is not an emergency in the United States, nor anywhere else outside of Africa.
Within Africa there is definitely cause for concern over monkeypox, because there people are actually dying from the virus. While the numbers might not rise to a level at which the term “emergency” becomes appropriate, neither is monkeypox’ mortality in Africa something that should be blithely ignored.
Are the virtue signallers over monkeypox worried about people dying in Africa? No. The virtue signallers are worried about sex clubs in Los Angeles potentially closing. The virtue signallers are worried about gay and bisexual men being told to refrain from anonymous sex with multiple partners.
Somehow, inconveniencing gay and bisexual men with an expectation of responsibility and self control is an outrageous display of discrimination, but turning away and ignoring monkeypox deaths in Africa is of no consequence.
Yet I am not shocked by this—not any more.
I am not surprised by this—not any more.
I am disturbed by this, and I am saddened by this. People can be—and should be—better than this. People certainly deserve better than this, whether in Africa or beyond Africa.
However, to keep this from being relentlessly ponderous, depressing, and even dreary, I shall close with a little ditty from Tom Lehrer to illustrate the absurdity of all the virtue signalling.
All Facts Matter is a reader-supported publication. To receive new posts and support my work, consider becoming a free or paid subscriber. Alternatively, please consider leaving a tip through Ko-Fi. Thank you always for your support!
A word’s “denotative” meaning—literally the “dictionary definition”—is the definition listed first in the dictionary. Subsequent “connotative” meanings, when listed in a dictionary, are listed after the denotative meaning.





So we’ll written, FACTUAL and on point !
I will send this around to dispel the fear propaganda pushers.
Thank you for setting the record straight and clear.
The gay community should feel insulted that they aren't being trusted with taking responsibility. But there is no money in abstinence