

Three Graphs Showing The Abysmal Failure Of The COVID "Vaccines"
The Data Is Clear: The "Vaccines" Are Worthless

With Moderna seeking an Emergency Use Authorization (EUA) to push its mRNA COVID-19 “Vaccine” into the arms of little children and babies, it is once again imperative to stress one unequivocal undeniable unalterable fact: these “vaccines” do not work.
The “vaccines” have never worked.
The “vaccine” studies and trials claiming to show otherwise are garbage.
The data—taken at face value and without equivocation or rationalization—does not admit of any other option.
The mRNA “Vaccines” Are NOT Vaccines
Before I continue, we must clarify the language.
Calling the mRNA shots “vaccines” is only appropriate if one accepts the CDC’s stealth redefinition of the term “vaccine” within their website (and thus their public communications on the topic).
Prior to September 1, 2021, the CDC’s website defined a vaccine as something that provided “immunity” to disease.
Vaccine: A product that stimulates a person’s immune system to produce immunity to a specific disease, protecting the person from that disease. Vaccines are usually administered through needle injections, but can also be administered by mouth or sprayed into the nose.
Under this definition, “immunity” meant freedom from infection.
Immunity: Protection from an infectious disease. If you are immune to a disease, you can be exposed to it without becoming infected.
After September 1, 2021, the CDC changed the definition of a vaccine to something that only provides “protection”.
Vaccine: A preparation that is used to stimulate the body’s immune response against diseases. Vaccines are usually administered through needle injections, but some can be administered by mouth or sprayed into the nose.
Vaccination: The act of introducing a vaccine into the body to produce protection from a specific disease.
The difference is subtle and yet profound. On August 31, 2021, a vaccine provided immunity, and thus prevented infection. On September 1, 2021, a vaccine only stimulated the immune system to “produce protection”—meaning it does not prevent infection.
Why did the CDC feel the need to change the definition? As is documented by the CDC’s own internal emails, excellently summarized by the folks at TechnoFog, they realuzed the previous definition was “problematic” when applied to the Pfizer and Moderna mRNA preparations.
The solution: change the definition. And, just like that, what wasn't a vaccine because it didn't provide immunity became a vaccine because it provided protection.
Even The New Definition Is Problematic
Unfortunately for the advocates of the mRNA “vaccine” technology, even the new definition is problematic. If we accept that a “vaccine” provides “protection”, then, when we look at the data, we should see a demonstration of that protection.
We do not.
When we examine excess mortality data for the United States during the COVID-19 pandemic, both before and after the introduction of the “vaccines”, the trends are unmistakable, and unequivocally damning against the mRNA “vaccines”. As the percentage of the US population that is counted as fully vaccinated increased, excess mortality also increased. “Vaccine” efficacy should have shown a decrease in excess mortality and that we do not see.
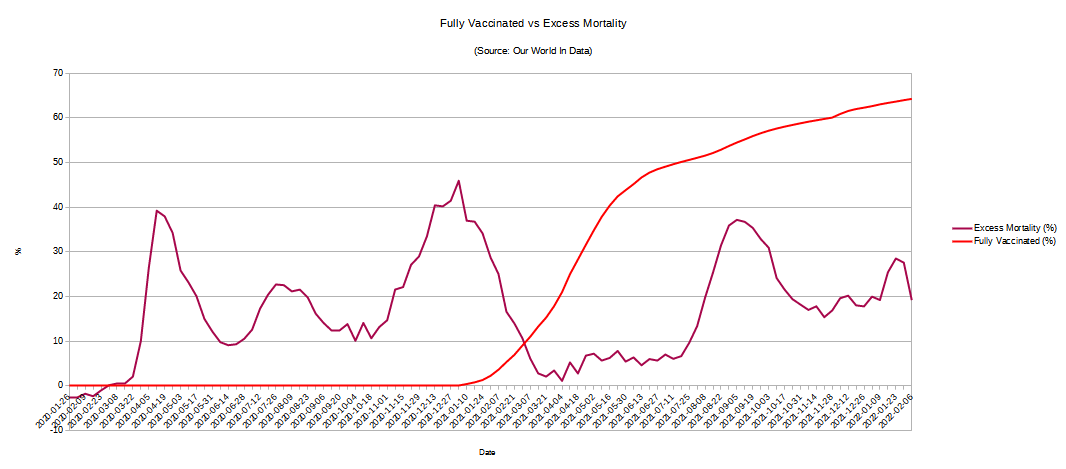
The late-summer spike in excess mortality, occurring after over 50% of the US population was “fully vaccinated”, is incompatible with the “vaccines” providing protection. Protected people do not die.
Nor can that spike be attributed simply to the “unvaccinated”. The previous excess mortality peak, at 45.92% on January 3, 2021, is just 8 points higher than the late summer peak of 37.16% on September 5, 2021. With half the country (54.64%) “fully vaccinated”, for that excess mortality to be attributed to unvaccinated patients exclusively would require a more virulent strain of the SARS-CoV-2 virus. However, by September of 2021, the dominant COVID-19 strain was the Delta variant, universally reported as less virulent.
From the New York Times in July:
After the Alpha variant began spreading late last year, many people assumed that it was both more contagious and more severe. The data soon told a different story, though: Alpha seems to be only more contagious.
Now the story may be repeating itself with Delta. It is significantly more contagious than even Alpha by almost every measure. It does not appear to be more severe, based on the data available so far.
From the New York Post, also in July:
The seven-day average of new UK cases is above 25,000, the highest since late January, when the weekly average had just dropped from a peak of 50,000. But only 2,000 COVID cases are hospitalized, vs. nearly 40,000 in January. Daily deaths average under 20, vs. more than 1,000 in January.
Similarly: Israel, despite a spike in Delta cases, is seeing deaths in the single digits over the last month.
In other words, Delta looks to be less lethal than previous variants, despite media scare stories.
With less virulent strains of the virus in circulation, the only way to get to a 37% spike in excess mortality during a pandemic, when over 50% of the population is “vaccinated” and therefore “protected”, is for the “vaccines" to not work.
Much Of the Excess Mortality Is COVID Related
For those hoping to explain the post-vaccination excess death spike as unrelated to the COVID-19 pandemic, prepare to be disappointed: the case numbers do not allow that.
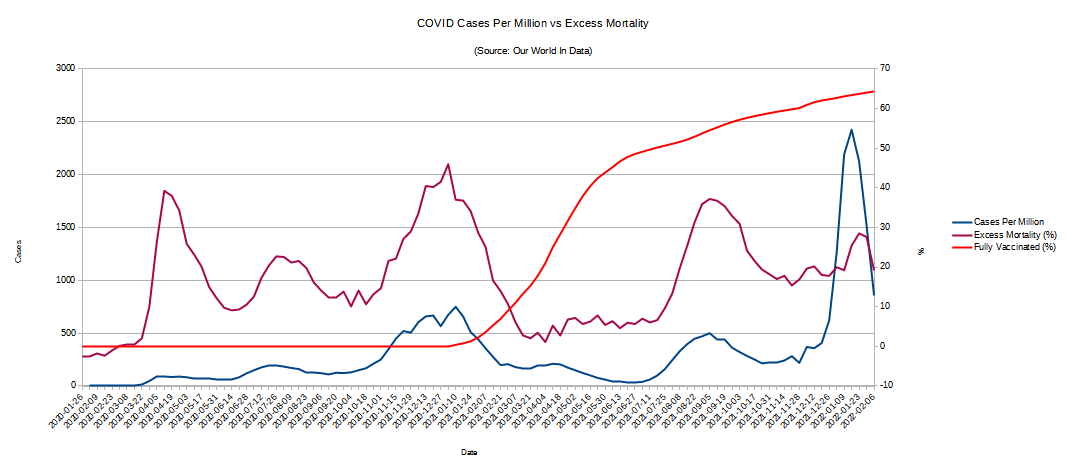
As this second graph illustrates, COVID cases per million in the US (left axis) and excess mortality percentages in the US (right axis) fluctuate more or less in tandem. Moreover, the worst post-vaccination case peaks occur again after the vaccination rate exceeded 50%.
Keep in mind that excess mortality is just that—the amount of deaths over and above the historical norm.
Excess mortality is a term used in epidemiology and public health that refers to the number of deaths from all causes during a crisis above and beyond what we would have expected to see under ‘normal’ conditions.
When each rise in daily COVID-19 case counts produces a corresponding rise in excess deaths, the inevitable conclusion to be drawn is the two phenomenon are related. COVID cases lead to excess death.
Moreover, with over 50% of the population “vaccinated”, if the “vaccines” worked, the coincidental late summer rise in both COVID cases and excess death should not have happened.
Just in case one is still skeptical, there is the third graph, of COVID deaths per million data, which shows the same relationship.
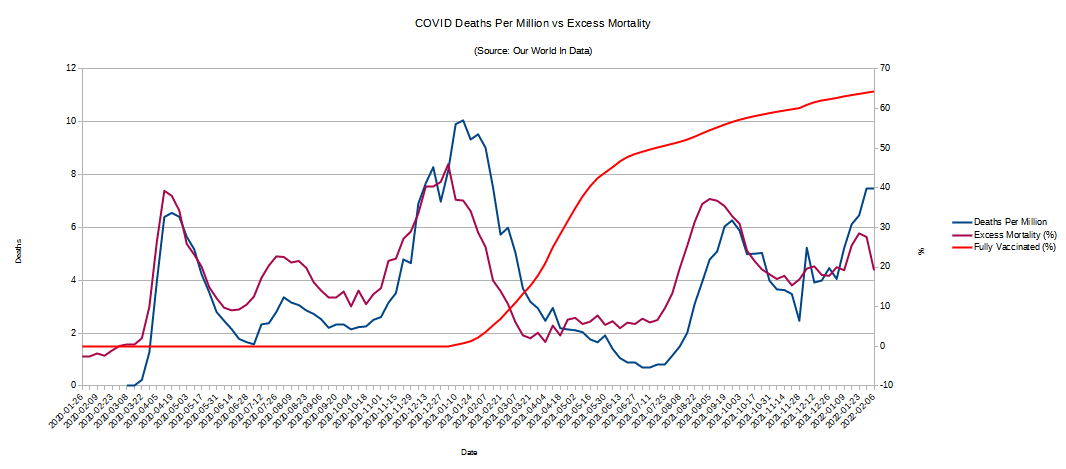
These are unmistakable trends linking COVID cases and deaths to excess mortality before and after the introduction of the mRNA “vaccines”.
Where is the “protection”? The data does not show it.
Where is the benefit? The data indicates there is none.
But…The “Science”
What, then, do we say to the studies touted by the CDC as demonstrating the efficacy of the “vaccines”? To be sure, there are many such studies:
Are all these studies wrong? In a word, yes.
There is no mistaking death. There is no conflating death with any other pathological condition. There is no need for a PCR test to diagnose death.
Moreover, the “science” surrounding the SARS-CoV-2 virus, the COVID-19 pandemic, and in particular the “vaccines”, has always been tainted by anomalous interpretations.

Nor should we forget the eagerness of the “vaccine” vendors to make mountains out of molehills, making sweeping and broad claims on the thinnest of results.
It should therefore come as no surprise that the CDC is promoting medical propaganda—junk science instead of actual science.
All Facts Matter
Any and all studies of any phenomenon must explain all the data to be valid. Any study touting the efficacy of the “vaccines” must explain the excess mortality data. Any study which cannot do so is flawed and of only minimal utility, to be taken with a grain of salt. The fact that all studies promoted by the CDC ignore the excess mortality data is merely further evidence of the extent to which the “experts” have chosen to abandon the skeptical rational inquiry into the world that is actual science in favor of the latest incarnation of ideologically-driven scientific bastardy, which I call Faucism.
Yet the data remains the data. The facts remain the facts. Faucism cannot change the facts any more than Canute could command the tides (although, to his credit, Canute realized this, while the Faucists have yet to learn that lesson).
These “vaccines” have not stopped the pandemic as promised.
These “vaccines” have not prevented illness and death as promised.
These “vaccines” should be recalled.
The Emergency Use Authorizations by which these “vaccines” are being pumped into people's arms need to be canceled forthwith. They should not be expanded to include small children and babies.
England data: Office of National Statistics, Age-standardised mortality rates, 2021.
If you have a Telegram account, I can send it to you.
Have you looked at all cause mortality data from other countries?
England, Israel, Scotland, Canada?
These countries are ahead of the USA in terms of percentage of the population “fully vaxxed” / boostered, also ramped up prior to the USA (months earlier).
I looked at all cause mortality from England last autumn, it was eye-opening. Deaths increased post-vax campaign. Notable was the breakdown by age demographics: far younger sub-population succumbed than during the 2020 COVID-19 waves.
While some deaths are likely due to ‘societal’ factors (violence, alcoholism, drug abuse, crime, etc.), probably exacerbated by the lockdowns and aggressive masking policies, there could be a relation to the inoculations themselves. One needs to dig into the details.
I personally believe autopsies must be performed on all “unexpected, untimely, anomalous, surprising” deaths going forward.