

Yet More Proof That "Expert" Is Wokespeak for "Blithering Idiot"
Yes, You CAN Assess Your Own Personal Risk From COVID-19

Trigger warning: When I see rank stupidity being paraded as “expertise”, I get triggered.
As you might imagine, thanks to the Pandemic Panic Narrative, I get triggered a lot. Well, not so much these days, because my expectations for medical “experts”, while never very high, has fallen pretty much to zero. If they don’t have facts, evidence, and data, I can pretty much guarantee that I will not be impressed by what they have to say. If they stand on their credentials, I can absolutely guarantee that I will not be impressed one bit by what they have to say. Show me the data or shut the Hell up.
Yet even with my lowered expectations of “experts”, when an “expert” proceeds to write an entire article devoted to personal power whining, it’s still annoying. Whining is never a good look for intellectual leaders (what “experts” used to be back when expertise involved having more than three active brain cells). When I stumble across an essay by one Malia Jones, an “epidemiologist” at the University of Wisconsin, making the demonstrably false and foolish assertion that personal risk assessment for COVID-19 is “impossible”, it moves beyond annoying into the downright infuriating. Right now, I’m downright infuriated.

Individualized risk assessment is not a reasonable ask, even for someone who does risk assessment for a living, let alone for the rest of us. It's impossible to evaluate our own risk for any given situation, and the impossibility of the task can make us feel like giving up entirely. So instead of doing that, I suggest focusing on risk reduction. Reframing in this way brings us back to the realm of what we can control and to the tried and true evidence-based strategies: wearing masks, getting vaccinated and boosted, avoiding indoor crowds and improving ventilation.
At this point just about every working American has encountered some form of COVID protocol in the workplace—face masks, temperature checks, et cetera. Anyone who has flown or used public transportation has encountered the demonstrably unscientific demand that one must wear a mask to do so.
Regardless of the actual utility or mitigation effect of such measures, each of them is the result of some measure of risk assessment. For each such measure put into place, someone contemplated the situation presented by the COVID-19 pandemic, made an assessment as to what the proximate risks were from the pandemic, and what would be an effective mitigation against those risks. A risk assessment process is inevitable because without something in the way of risk assessment, one cannot even conceive of what mitigations to suggest or mandate.
This is not to suggest the risk assessment behind a mask mandate was well done. In LA, for example, the risk assessment was admitted to being along the lines of “the CDC says do it so we’ll do it.”

For public schools in Allegheny County, Pennsylvania, the risk assessment process involved ignoring CDC guidance to use local data and using the CDC’s own erroneous COVID severity level metric for the county.
Yet public officials in both LA and Pittsburgh firmly believed they were reducing risk for their respective cities. They were not, of course, because their risk assessment protocol was more a dereliction of duty than a serious cognitive effort, yet the fact of that belief establishes that some measure of risk assessment was undertaken.
In sum, every one of us is surrounded by COVID-19 risk assessments and their results, for better or for worse.
Individual Risk Assessments Are Not Merely Necessary, They’re Unavoidable
Two words suffice to demonstrate the lunacy of a presumed “epidemiologist” saying that individual risk assessments are impossible: Defensive Driving. The principles behind the concept of defensive driving are little more than a dynamic cyclical process of risk assessment and risk mitigation while operating a motor vehicle (emphasis mine).
Different industries and workplace environments contain varying degrees of risk; for example, operating a commercial motor vehicle (CMV) or commuting between worksites are legitimate contingencies for accidents to occur on the job, drawing on defensive driving skills to reduce liabilities. Employers must coordinate a safe driving culture among their workforce, incorporating defensive driving into the framework of health and safety guidelines for CMV operators, among other personnel where traveling is secondary to typical job requirements.
While rarely presented in terms of risk assessment and risk mitigation, the goal of defensive driving is easily seen as risk mitigation, and the practice of defensive driving involves constantly assessing risks on the road in order to determine how best to mitigate those risks.
Thus, not only is individual risk assessment quite possible, it is as a concept as ubiquitous as cars themselves.
People can do individual risk assessment when they get behind the wheel of a car but cannot do individual risk assessment when faced with an infectious respiratory disease? That is what Ms. Malia Jones is effectively—and erroneously—stating.
People can make such assessments—and invariably do make such assessments every single day. When you decide to take the mask off now that they are no longer required on public transportation, you are assessing the risk of that action. Likewise, if you leave the mask on, you are assessing the risk of that action. In both of these actions, just as when you get behind the wheel of your car, you are assessing risk and making choices based on that assessment.
What a professional epidemiologist such as Ms. Malia Jones should be articulating is how to perform that risk assessment properly, so as to best mitigate potential risks and minimize the chances of both infection and severe illness.
What Is Risk Assessment?
The essence of any risk assessment process is simply identifying potential hazards and the harm that can arise from that hazard. As the risk assessment page at Ready.gov states:
A risk assessment is a process to identify potential hazards and analyze what could happen if a hazard occurs.
While Ready.gov uses the language primarily of risks to property, if one pauses to realize that personal health is always among one’s most valuable “assets”, the utility of the articulated process is quite apparent.
As you conduct the risk assessment, look for vulnerabilities—weaknesses—that would make an asset more susceptible to damage from a hazard. Vulnerabilities include deficiencies in building construction, process systems, security, protection systems and loss prevention programs. They contribute to the severity of damage when an incident occurs. For example, a building without a fire sprinkler system could burn to the ground while a building with a properly designed, installed and maintained fire sprinkler system would suffer limited fire damage.
Within a COVID risk assessment, “vulnerabilities” could be co-morbidities, or perhaps environmental concerns. Also, just as a fire sprinkler system is easily seen as a mitigation to fire risk in a building, a healthy immune system is easily seen as a mitigation to infectious disease in a person.
Returning to the defensive driving example above, the decision to slow down when driving on wet pavement or down a narrow subdivision street lined with cars is a response occasioned by the recognition of the hazards of slick driving conditions or of people running out suddenly from behind cars.
Workplace safety site Safetynotes.net articulates a fairly straightforward 5-step process of risk assessment (more precisely risk assessment and mitigation).
There are 5 steps to conduct a risk assessment:
Identify the hazard.
Assess the risk
Put controls/safe guards in place
Re-assess the risk with control in place.
Confirmation of reduced risk.
One thing to note about the process definitions and examples given both at Ready.gov and Safetynotes.net: they are generic rather than specific. These are not descriptors of particular hazards and their mitigations, but rather of the analytical process for both identifying hazards and determining what mitigations are appropriate in a given situation. Being generic, they are (and are intended to be) accessible by anyone, to be used by (hopefully) everyone.
Assessing COVID-19 Risk
While I have made the case multiple times that COVID-19 is neither as deadly nor as severe as the corporate media have asserted—particularly as regards the Omicron sub-variants—for the purposes of this article I am putting aside particular claims of risk regarding COVID-19. It is one thing to talk about the levels of danger as presented by broad epidemiological data, but quite another when assessing personal risk. Unlike the “experts”, my goal here is not to tell you that COVID-19 is or is not a threat to you specifically, or that you have either great risk or no risk of fatality from the disease. That would be an arrogant and absurd thing to do.
Rather, consider the known risk factors for COVID-19 as they apply to your particular medical situation. Consider how each risk factor might alter either your susceptibility to infection or potential for contracting a severe case of the disease. Then consider what you can do to mitigate those risks.
In one of its more useful moments, the CDC in 2020 assembled a list of potential risk factors for contracting COVID (or having it turn into a severe form of the disease).
Because COVID-19 is a new disease, more work is needed to better understand the risk factors for severe illness or complications. Potential risk factors that have been identified to date include:
Age
Race/ethnicity
Gender
Some medical conditions
Use of certain medications
Poverty and crowding
Certain occupations
Pregnancy
The CDC also highlights the significance of risk factors in determining how best to respond to the COVID pandemic.
It is important to learn about risk factors for severe COVID-19 illness because it can help you:
Take precautions as you go about your daily life and attend events.
Better understand how a medical condition could affect your own health if you get sick with COVID-19.
Anticipate medical treatment that you might need if you get sick.
Reduce your risk for severe COVID-19 illness by managing any conditions you have that are risk factors.
(Yes, I’m citing the CDC….irony abounds.)
By far the most significant risk factor one has with regards to SARS-CoV-2 infection is age. The older one gets, the more vulnerable one becomes, statistically speaking.
Older adults are at highest risk of getting very sick from COVID-19. More than 81% of COVID-19 deaths occur in people over age 65. The number of deaths among people over age 65 is 97 times higher than the number of deaths among people ages 18-29 years.
Other risk factors (not in order of greatest risk) include:
Cancer
Chronic Kidney Disease
Chronic Lung Diseases
Diabetes
Heart Disease
HIV infection
Obesity
The CDC also provides a list of mitigating actions one can take, and a few are even useful:
Wash your hands often
Cover coughs and sneezes
Monitor your health daily
There is another item I would add to the list of plausible mitigations: take your vitamins.
Added to the known risk factors and mitigations is the known level of COVID-19 in a particular area. The CDC provides county-specific monitoring of COVID-19 cases and deaths (New York County, New York, for example).
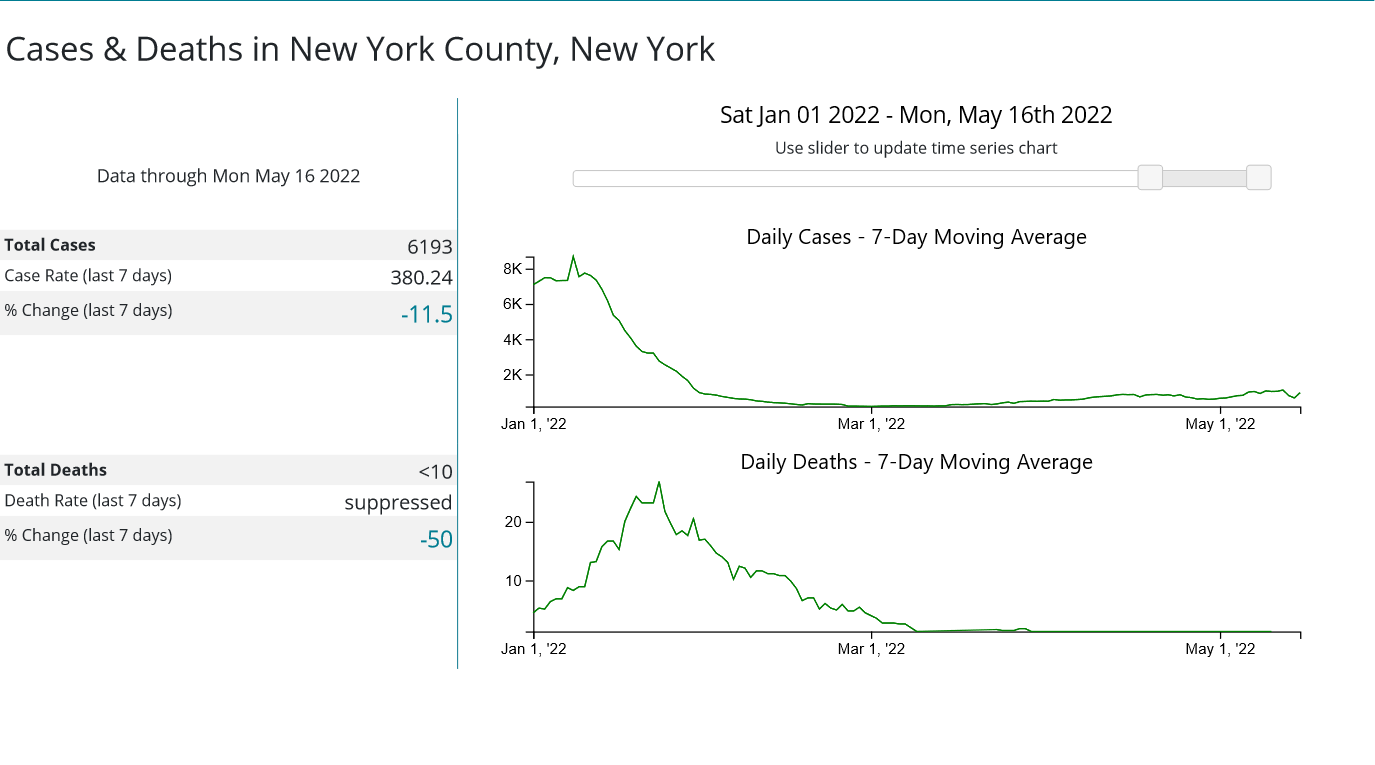
Hospitalization rates are also tracked by county.
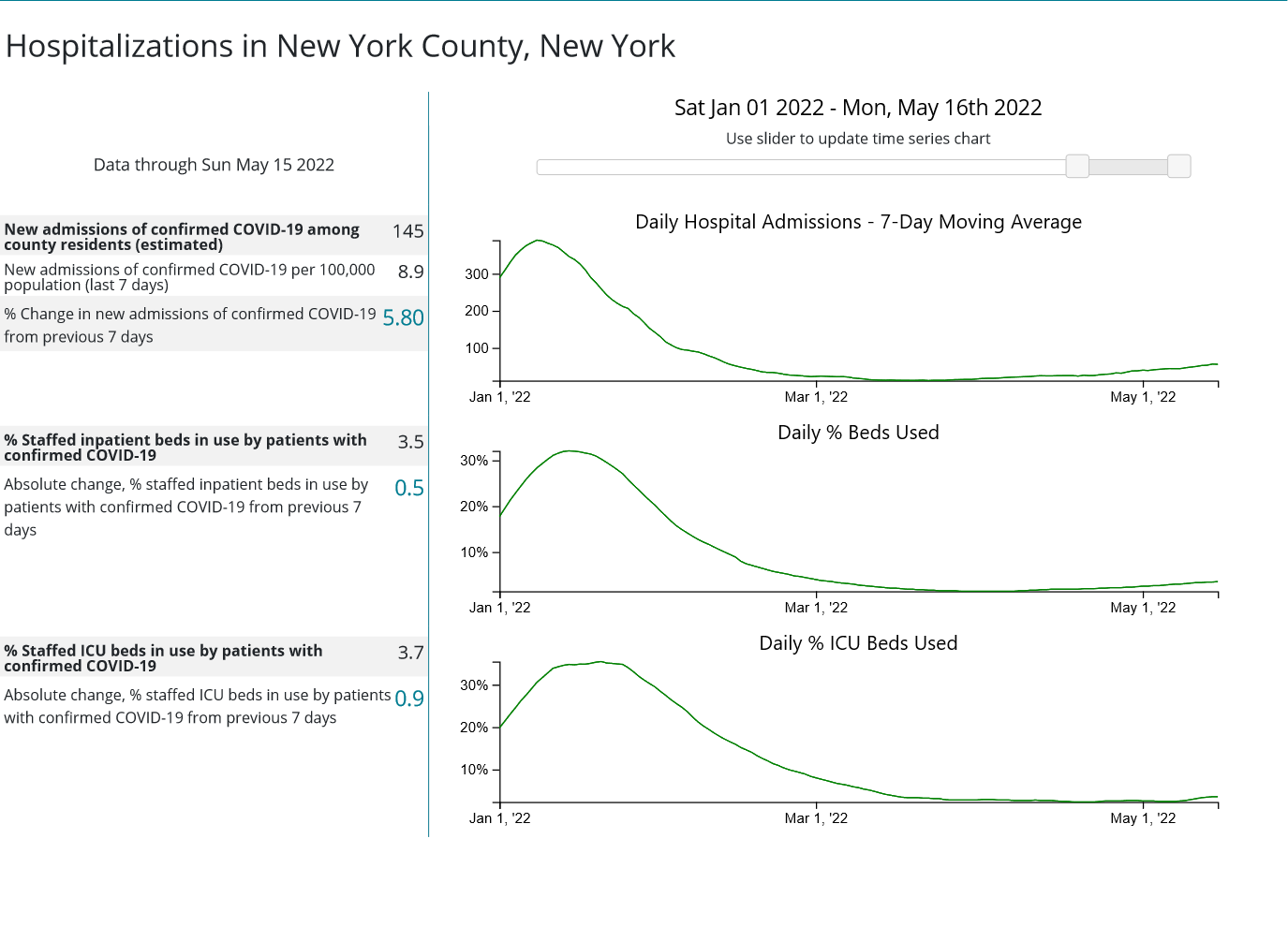
Similar data is almost always published by one’s state and/or local public health agency as well. A quick DuckDuckGo search of COVID-19 data for your area should suffice for finding the relevant data. Rising cases and/or hospitalizations indicate a greater prevalence of disease—and thus greater risk of exposure.
Armed with the above data, the actual risk assessment process itself I submit is fairly straightforward. The hazard is known: COVID-19. The risks are broadly identifiable: the greater the number of known risk factors and co-morbidities one has the greater the risk. Potential mitigations one can take to reduce the risk of infection and/or severe disease are broadly known: hand hygiene, good nutrition, personal health monitoring, et cetera.
Armed with the above data, anyone can assess for themselves their own vulnerability to COVID-19, and decide how best to address that risk. I will also point out that similar risk assessment is quite feasible for just about any infectious disease, and more broadly for any known safety hazard.
Not only can everyone perform such assessments for themselves, everyone should perform such assessments for themselves. You are always the best guardian of your personal health and safety. No one is better qualified to gauge your personal risks than you—it is your body, your health, and your life.
For an epidemiologist such as Malia Jones, of all people, to state that it is impossible for you to perform your own individual risk assessment is not merely absurd and false, it is an affront to the very science of epidemiology itself. The origins of epidemiology began in the efforts of one London physician, Dr. John Snow, to trace the origin of the 1854 London Cholera outbreak, which ultimately lead to the identification of a contaminated water pump. By disabling that water pump, so that Londoners would have to draw their water from elsewhere, the outbreak was effectively stopped.
While Dr. Snow proved that disease spread could be mapped and traced to determine how diseases spread, he also showed that changing personal habits can be quite effective at mitigating infectious disease. Anyone who avoided the contaminated pump in 1854 London was at much less risk for cholera, even before he persuaded the city to disable the pump. The entire thrust of epidemiology is to identify and articulate how diseases spread precisely so that people can take the individual actions necessary to reduce their risk of infection.
The actual severity and danger from the SARS-CoV-2 virus is and always will be a matter of some debate, as invariably is the case in all matters of health and physical well being. Yet there should be no debate over the capacity of individuals to manage their own health and take charge of their own health risks.
Any “epidemiologist” who says otherwise is no expert, but merely a blithering idiot and should be regarded as such.
“It is the pinnacle of arrogance to assume that whatever it is that “the experts” believe now is in fact the truth, the whole truth, and nothing but the truth. Scientists have believed and public health officials have promoted many wrong things over the years, for both honorable, and not so honorable reasons. Sometimes the public health message is dead wrong.”
― Heather E. Heying
Excellent work, Peter.
She needs to do a risk assessment on sounding like a brainwashed zombie.