

Face Masks: A Study In Science Denialism
Facts? Data? Evidence? Research? Pah...We've Got Mandates!

Los Angeles County is once again demonstrating its studied disregard for any type of scientific research, scientific data, scientific evidence, or anything involving scientific rigor when it comes to Los Angelenos’ favorite Faucist fetish, the face mask.
Yes, sports fans, LA is once again anticipating a return to masking. Because “COVID” (of course).

Indoor masking in public settings could return to Los Angeles County in a week as circulation of the hyper-infectious BA.5 Omicron subvariant continues to push coronavirus case counts higher and sends increasing numbers of people to the hospital.
Never mind that there is no evidence that masking has any impact on the spread of infectious respiratory diseases, including COVID-19. Disregard the data on the ground, or anything resembling critical analysis of that data. Just bleat out “COVID baaaaad. Masks gooood.”
That’s how public health policy is made in the City of Angels. And elsewhere (unfortunately).
What Does The Data Show?
First of all, what does it mean that coronvirus case counts are being pushed “higher”?
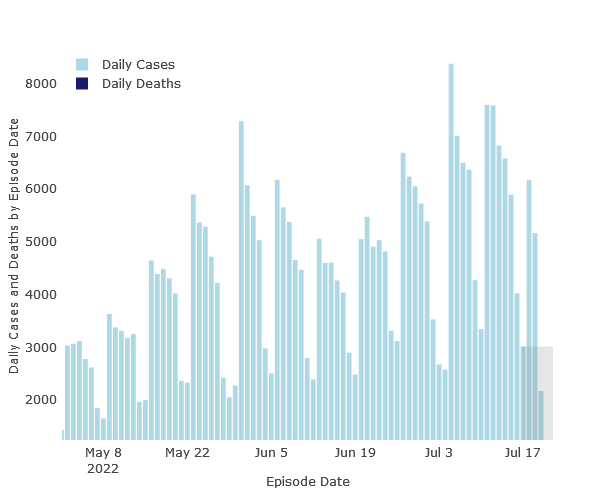
Here’s what it doesn’t mean: that the daily count of new cases is rising. It isn’t. As LA County’s own COVID dashboard illustrates, coronavirus case counts peaked in early July and have been falling.
To be fair, the dashboard does show that 1,247 people in Los Angeles County were hospitalized for COVID-19, and that number has risen since April.
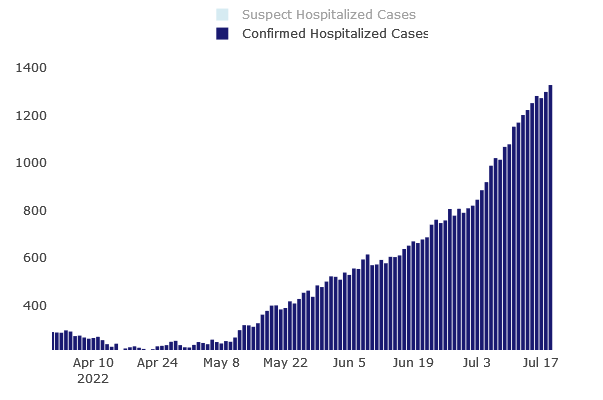
However, that is 1,247 hospitalizations out of a population of nearly 10 million (Los Angeles County is the larges county in the United States). That is 0.0126% of the total population. That’s not a public health crisis of any kind.
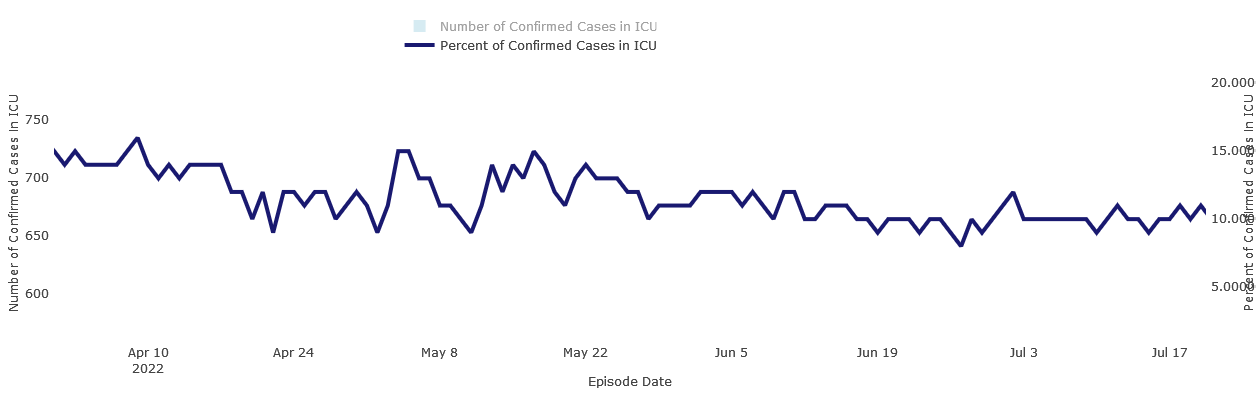
Moreover, the percentage of those cases in ICU has also declined recently, from 15% in April to 10% most recently.
That is what the data shows. Does this reconcile to the Los Angeles Times narrative of a "hyper-infectious BA.5 Omicron subvariant”? You decide.
Still No Evidence Mask Mandates Work
Remember, mask mandates were recently proven ineffective in yet another study, this time of North Dakota school districts1.
We observed no significant difference between student case rates while the districts had differing masking policies (IRR 0.99; 95% CI: 0.92 to 1.07) nor while they had the same mask policies (IRR 1.04; 95% CI: 0.92 to 1.16). The IRRs across the two periods were also not significantly different (p = 0.40). Our findings contribute to a growing body of literature which suggests school-based mask mandates have limited to no impact on the case rates of COVID-19 among K-12 students.
“Limited to no impact” is a four dollar way of saying “does not work.”
The North Dakota study joins the legion of other studies that show the same inefficacy (another four dollar term meaning “does not work”) of universal masking and mask mandates.
How large is that legion?
In April of 2020, I outlined four Random Controlled Trials involving face masks and Influenza Like Illness, all of which saw no statistically significant reduction in disease spread by universal masking strategies.

In August of last year, statistician Jeffrey H. Anderson dug a little deeper and found a total of 14 Random Controlled Trials which failed to produce reliable evidence of any benefit from universal mask mandates as a public health strategy.
Even the large Bangladeshi study which the CDC claimed showed positive impact fails to deliver on that claim when one looks closely at the data—which is what Denis Rancourt, researcher with the Ontario Civil Liberties Union in Canada did, and found the study “fatally flawed.”
The cluster-randomized trial study of Abaluck et al. (2021) is fatally flawed, and therefore of no value for informing public health policy, for two main reasons:
The antibody detection was performed using a single commercial FDA emergency-use-authorized (EUA) serology test that is not suitable for the intended application to SARS-CoV-2 in Bangladesh (not calibrated or validated for populations in Bangladesh; undetermined cross-reactivity against broad-array IgM antibodies, malaria, influenza, etc.).
The participants (individual level, family level, village level) in the control and treatment arms were systematically handled in palpably different ways that are linked to factors established to be strongly associated to infection and severity with viral respiratory diseases, in particular, and to individual health in general.
Once one looks at the entire data set, as statistician William Briggs also did, the demonstrated efficacy of face masks in that study was 0.0026%.
Which means there are at least fifteen Random Controlled Trials which show “limited to no impact” for universal masking strategies.
Face mask mandates do not work against infectious respiratory disease.
Given the high regard accorded the Random Controlled Trial by scientific researchers, how is it that Los Angeles County persists in its thinking that face masks are at all effective against infectious respiratory disease?
The Faucist Fetish Is Persistent
Nor is this the first time in recent months that LA County has flirted with universal masking mandates. They were at this very juncture just this past April.
They are also hardly an isolated instance of the Faucist fetish for face masks.
Philadelphia had a ten-day flirtation with the mask mandate in April as well.
Allegheny County, Pennsylvania reinstated the mask mandate for its public schools just this past May.
Half of North Carolina counties advise people to wear masks in public. Because “Omicron”—and because the CDC persists in ignoring the research summarized above in order to claim that face masks are effective when they really aren’t.
As the new BA.5 subvariant surges through the state, nine counties transitioned from a medium- to a high-risk classification this week, bringing the total number of high-risk counties to 50. In those areas, the CDC recommends that people wear a well-fitting mask in indoor, public places, regardless of vaccination status.
Independent research and critical analysis of scientific data—exactly what the CDC, as a “science-based, data-driven, service organization“, should be doing—show the CDC’s recommendation is nothing but hogwash and horse hockey.
Such is the dogged persistence of the Faucist fetish for face masks, that it can withstand a constant barrage of facts and evidence against it.
CDC Opinions Are Just That: Opinion. Not Fact
One point must be stressed over and over again, if it is to have any chance at punching through the corporate media’s Pandemic Panic Narrative on face masks: CDC recommendations are opinion, not fact. As such, they are the worst form of evidence. Even the “experts” concede this—as they did in a 2018 meta-analysis of clinical practice guidelines2, which clearly ranked even expert opinions well below direct empirical data.
Accordingly, CDC recommendations, in order to have even the slightest of value, must reconcile with existing research and evidence. In the same vein, anyone who is guided by CDC recommendations must also be familiar with at least some of the existing research and evidence, or they are not making proper use of the recommendations.
That’s how science—actual scientific research and inquiry, not “The Science™” worshipped by Anthony Fauci and others—is done in the real world. That’s how science properly informs public policy: weigh recommendations in light of the available research. That’s how public policy can be kept grounded in reailty, rather than getting lost in the weeds of foolish ideology.
If someone wants to wear a face mask while out in public, or even alone in his or her car, let them. They should have that right.
By the same token, everyone who understands that the overwhelming volume of scientific data shows the face mask to be nothing more than a security blanket should have the right to dispense with the mask.
That’s how choice works. That’s what you get when people make informed choices using facts, evidence, and data, as opposed to propaganda and ideology.
Neeraj Sood, Shannon Heick, Josh Stevenson et al. Association between School Mask Mandates and SARS-CoV-2 Student Infections: Evidence from a Natural Experiment of Neighboring K-12 Districts in North Dakota, 01 July 2022, PREPRINT (Version 1) available at Research Square [https://doi.org/10.21203/rs.3.rs-1773983/v1]
Ponce, O. J., et al. “What Does Expert Opinion in Guidelines Mean? A Meta-Epidemiological Study.” BMJ Evidence-Based Medicine, vol. 22, no. 5, 2017, pp. 164–69.
MASKS.....The lack of oxygen to the brain makes lots of people LOVE them.... also virtue signaling is at an all time high right now....
The mask peddling from 'experts' who know this is bull shit is irritating as it is troubling.